

Basal Cisternostomy for Severe TBI: Surgical Technique and Cadaveric Dissection
- PMID: 35599786
- PMCID: PMC9120838
- DOI: 10.3389/fsurg.2022.915818
Basal Cisternostomy for Severe TBI: Surgical Technique and Cadaveric Dissection
Erratum in
-
Erratum: Basal cisternostomy for severe TBI: Surgical technique and cadaveric dissection.Front Surg. 2023 Mar 22;10:1183723. doi: 10.3389/fsurg.2023.1183723. eCollection 2023. Front Surg. 2023. PMID: 37035558 Free PMC article.
Abstract
Introduction: Cisternostomy is emerging as a novel surgical technique in the setting of severe brain trauma. Different surgical techniques have been proposed with a variable degree of epidural bone work. We present here the surgical technique as it is currently performed in our Institution.
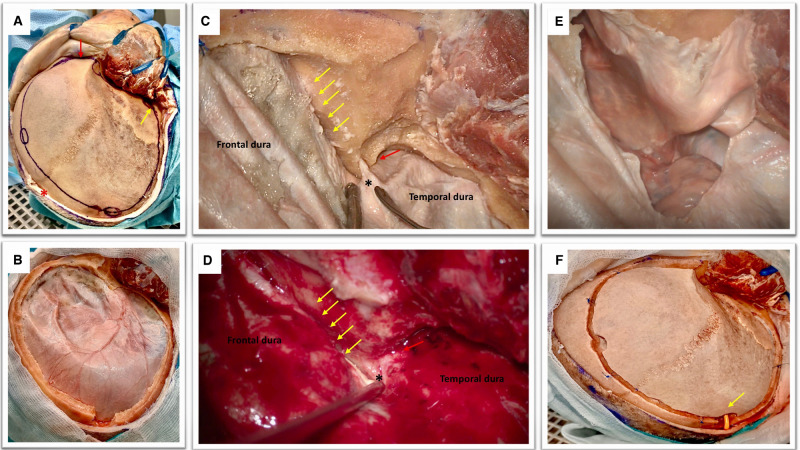
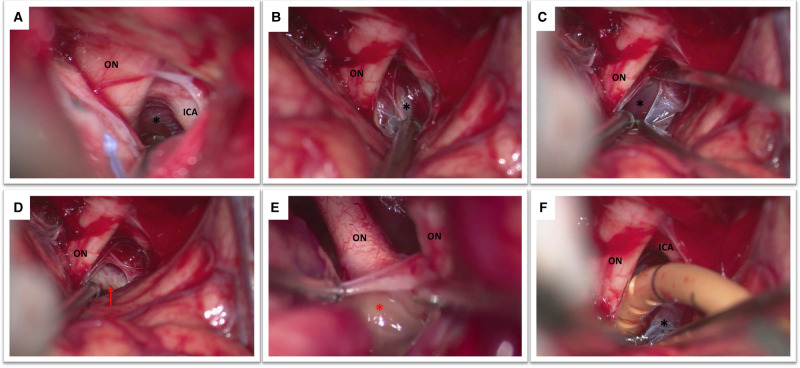
Methods: Anatomical dissection of one adult cadaveric head, injected and non-formalin fixed was perfomed. A large right fronto-temporo-parietal craniotomy was accomplished. Extradural sphenoidal drilling till opening of the superior orbital fissure was performed. The microsurgical anatomy of basal cisternostomy was then explored.
Results: A step by step description of the surgical technique, enriched with cadaveric and intraoperative images, was made.
Conclusion: Basal cisternostomy is a promising surgical technique that does not necessarily include complex surgical maneuvers. Trained neurosurgeon can safely implement it in their clinical practice.
Keywords: cadaveric dissection; cisternostomy; decompressive craniectomy (DC); severe brain trauma; skull base.
Copyright © 2022 Giammattei, Starnoni, Messerer and Daniel.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources