

Paediatric critical COVID-19 and mortality in a multinational prospective cohort
- PMID: 35599855
- PMCID: PMC9111167
- DOI: 10.1016/j.lana.2022.100272
Paediatric critical COVID-19 and mortality in a multinational prospective cohort
Abstract
Background: To understand critical paediatric coronavirus disease 2019 (COVID-19) and evaluate factors associated with mortality in children from high and low-middle income countries.
Methods: Prospective, observational study of critically ill children hospitalised for COVID-19 in 18 countries throughout North America, Latin America, and Europe between April 1 and December 31, 2020. Associations with mortality were evaluated using logistic regression.
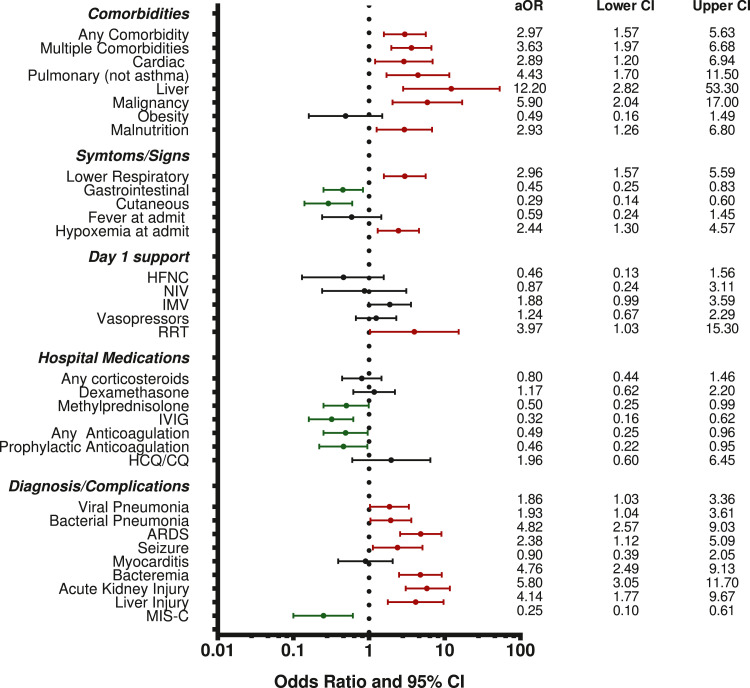
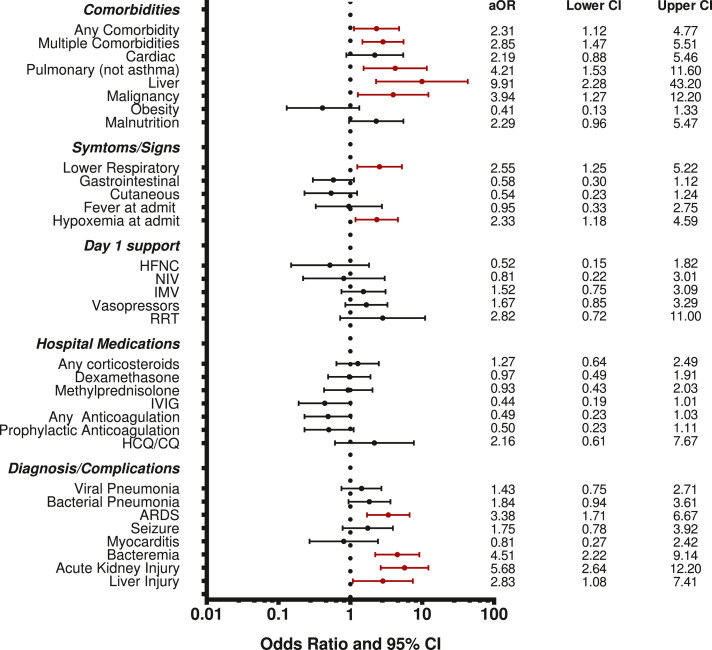
Findings: 557 patients (median age, 8 years; 24% <2 years) were enrolled from 55 sites (63% Latin American). Half had comorbidities. Invasive (41%) or non-invasive (20%) ventilation and vasopressors (56%) were the most common support modalities. Hospital mortality was 10% and higher in children <2 years old (15%; odds ratio 1·94, 95%CI 1·08-3·49). Most who died had pulmonary disease. When adjusted for age, sex, region, and illness severity, mortality-associated factors included cardiac (aOR 2·89; 95%CI 1·2-6·94) or pulmonary comorbidities (aOR 4·43; 95%CI 1·70-11·5), admission hypoxemia (aOR 2·44; 95%CI 1·30-4·57), and lower respiratory symptoms (aOR 2·96; 95%CI 1·57-5·59). MIS-C (aOR 0·25; 95%CI 0·1-0·61) and receiving methylprednisolone (aOR 0·5; 95%CI 0·25-0·99), IVIG (aOR 0·32; 95%CI 0·16-0·62), or anticoagulation (aOR 0·49; 95%CI 0·25-0·95) were associated with lower mortality although these associations might be limited to children >2 years old.
Interpretation: We identified factors associated with COVID-19 mortality in critically ill children from both high and low-middle income countries, including higher mortality with younger age and COVID-related pulmonary disease but lower mortality in MIS-C. Further research is needed on optimal treatments for younger children and respiratory failure in paediatric COVID-19.
Funding: None.
Keywords: COVID-19; Epidemiology; Mortality; Outcomes; Paediatric intensive care unit.
© 2022 The Author(s).
Conflict of interest statement
No authors have any conflicts of interest to disclose
Figures
References
-
- Wang JG, Zhong ZJ, Mo YF, Wang LC, Chen R. Epidemiological features of coronavirus disease 2019 in children: a meta-analysis. Eur Rev Med Pharmacol Sci. 2021;25(2):1146–1157. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
