

Risk factors for SARS-CoV-2 seroprevalence following the first pandemic wave in UK healthcare workers in a large NHS Foundation Trust
- PMID: 35600250
- PMCID: PMC9091808
- DOI: 10.12688/wellcomeopenres.17143.3
Risk factors for SARS-CoV-2 seroprevalence following the first pandemic wave in UK healthcare workers in a large NHS Foundation Trust
Abstract
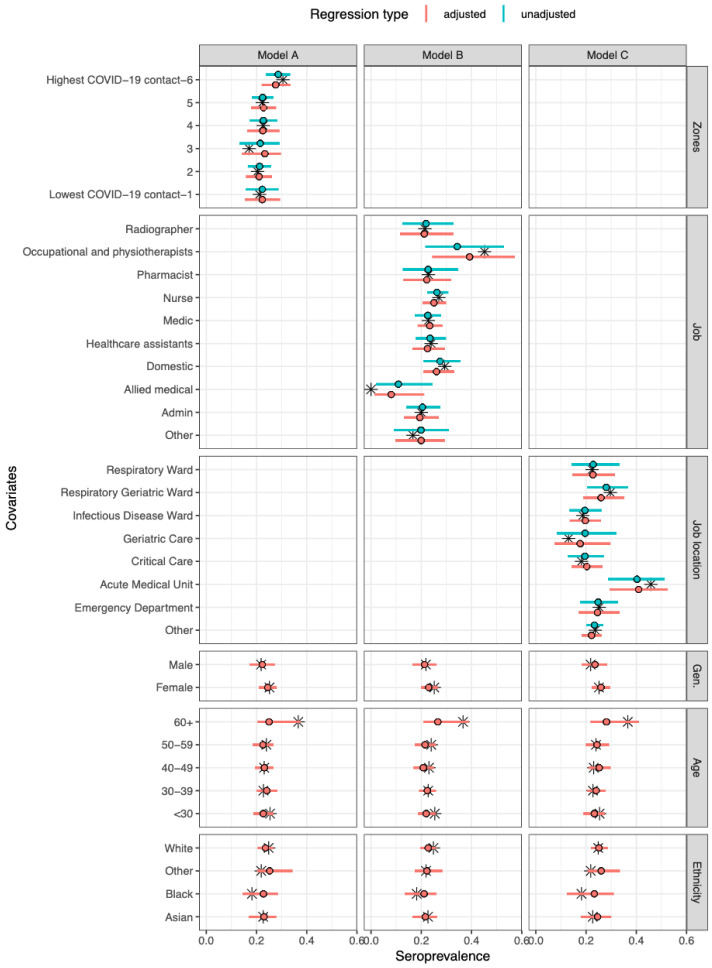
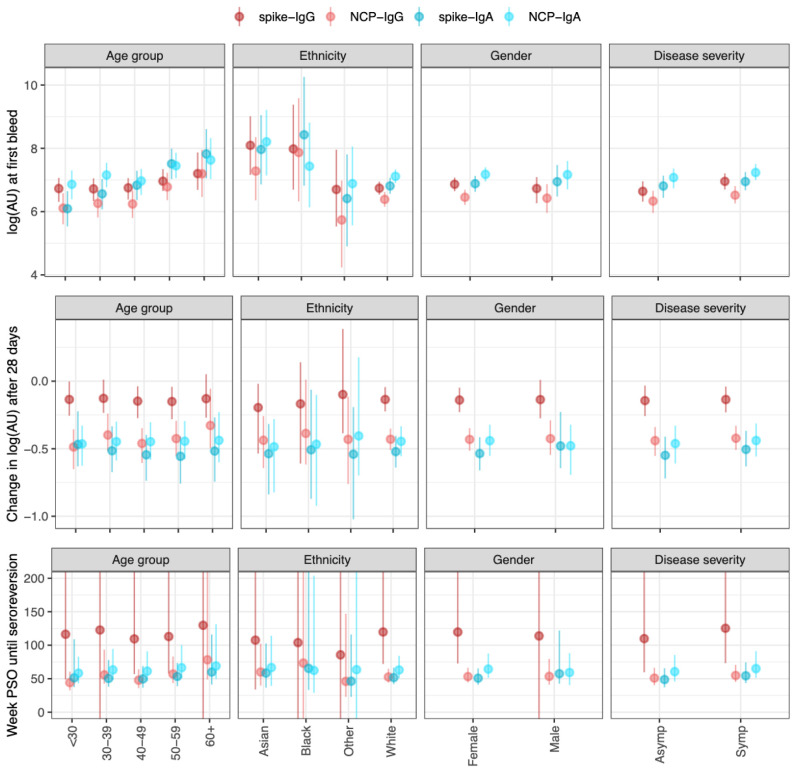
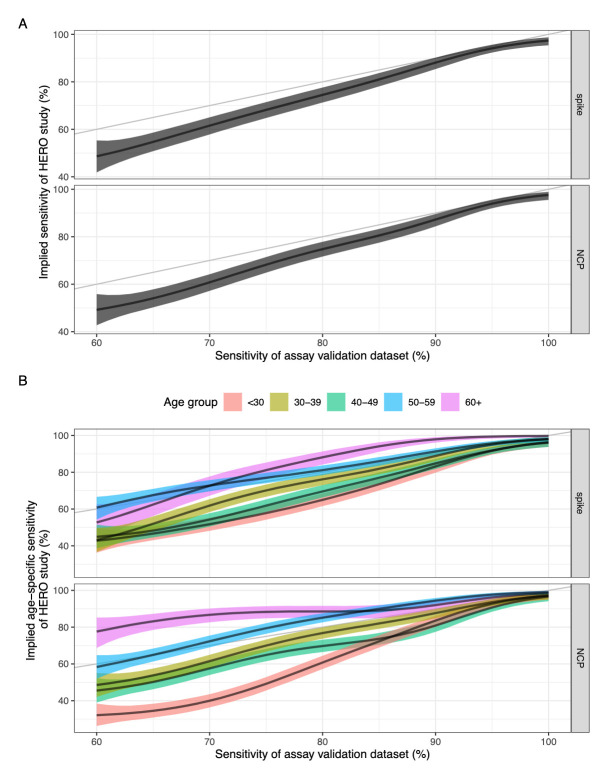
Background: We aimed to measure SARS-CoV-2 seroprevalence in a cohort of healthcare workers (HCWs) during the first UK wave of the COVID-19 pandemic, explore risk factors associated with infection, and investigate the impact of antibody titres on assay sensitivity. Methods: HCWs at Sheffield Teaching Hospitals NHS Foundation Trust were prospectively enrolled and sampled at two time points. We developed an in-house ELISA for testing participant serum for SARS-CoV-2 IgG and IgA reactivity against Spike and Nucleoprotein. Data were analysed using three statistical models: a seroprevalence model, an antibody kinetics model, and a heterogeneous sensitivity model. Results: Our in-house assay had a sensitivity of 99·47% and specificity of 99·56%. We found that 24·4% (n=311/1275) of HCWs were seropositive as of 12th June 2020. Of these, 39·2% (n=122/311) were asymptomatic. The highest adjusted seroprevalence was measured in HCWs on the Acute Medical Unit (41·1%, 95% CrI 30·0-52·9) and in Physiotherapists and Occupational Therapists (39·2%, 95% CrI 24·4-56·5). Older age groups showed overall higher median antibody titres. Further modelling suggests that, for a serological assay with an overall sensitivity of 80%, antibody titres may be markedly affected by differences in age, with sensitivity estimates of 89% in those over 60 years but 61% in those ≤30 years. Conclusions: HCWs in acute medical units and those working closely with COVID-19 patients were at highest risk of infection, though whether these are infections acquired from patients or other staff is unknown. Current serological assays may underestimate seroprevalence in younger age groups if validated using sera from older and/or more severe COVID-19 cases.
Keywords: Seroprevalence; antibody; Healthcare Worker; SARS-CoV-2; COVID; modelling; age; risk.
Copyright: © 2022 Colton H et al.
Conflict of interest statement
No competing interests were disclosed.
Figures
Similar articles
-
Risk factors for SARS-CoV-2 seroprevalence following the first pandemic wave in UK healthcare workers in a large NHS Foundation Trust.medRxiv [Preprint]. 2021 Jul 8:2021.07.07.21260151. doi: 10.1101/2021.07.07.21260151. medRxiv. 2021. Update in: Wellcome Open Res. 2021 Sep 3;6:220. doi: 10.12688/wellcomeopenres.17143.1. PMID: 34268521 Free PMC article. Updated. Preprint.
-
Seroprevalence of SARS-CoV-2 antibodies among healthcare workers in Dutch hospitals after the 2020 first wave: a multicentre cross-sectional study with prospective follow-up.Antimicrob Resist Infect Control. 2023 Nov 29;12(1):137. doi: 10.1186/s13756-023-01324-x. Antimicrob Resist Infect Control. 2023. PMID: 38031155 Free PMC article.
-
Seroprevalence of neutralizing antibodies to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) among healthcare workers in Makkah, Saudi Arabia.J King Saud Univ Sci. 2021 May;33(3):101366. doi: 10.1016/j.jksus.2021.101366. Epub 2021 Feb 13. J King Saud Univ Sci. 2021. PMID: 33613011 Free PMC article.
-
Seroprevalence and longevity of SARS-CoV-2 nucleocapsid antigen-IgG among health care workers in a large COVID-19 public hospital in Saudi Arabia: A prospective cohort study.PLoS One. 2022 Aug 12;17(8):e0272818. doi: 10.1371/journal.pone.0272818. eCollection 2022. PLoS One. 2022. PMID: 35960736 Free PMC article.
-
Seroprevalence of SARS-CoV-2 antibodies and associated factors in healthcare workers: a systematic review and meta-analysis.J Hosp Infect. 2021 Feb;108:120-134. doi: 10.1016/j.jhin.2020.11.008. Epub 2020 Nov 16. J Hosp Infect. 2021. PMID: 33212126 Free PMC article.
Cited by
-
Unsupervised machine learning to investigate trajectory patterns of COVID-19 symptoms and physical activity measured via the MyHeart Counts App and smart devices.NPJ Digit Med. 2023 Dec 22;6(1):239. doi: 10.1038/s41746-023-00974-w. NPJ Digit Med. 2023. PMID: 38135699 Free PMC article.
-
The German Translation of the Stress and Anxiety to Viral Epidemics-9 (SAVE-9) Scale: Results from Healthcare Workers during the Second Wave of COVID-19.Int J Environ Res Public Health. 2021 Sep 5;18(17):9377. doi: 10.3390/ijerph18179377. Int J Environ Res Public Health. 2021. PMID: 34501967 Free PMC article.
-
Greater preservation of SARS-CoV-2 neutralising antibody responses following the ChAdOx1-S (AZD1222) vaccine compared with mRNA vaccines in haematopoietic cell transplant recipients.Br J Haematol. 2024 Dec;205(6):2206-2218. doi: 10.1111/bjh.19874. Epub 2024 Nov 17. Br J Haematol. 2024. PMID: 39551718 Free PMC article.
-
Clinical usefulness of testing for severe acute respiratory syndrome coronavirus 2 antibodies.Eur J Intern Med. 2023 Jan;107:7-16. doi: 10.1016/j.ejim.2022.11.009. Epub 2022 Nov 10. Eur J Intern Med. 2023. PMID: 36379820 Free PMC article. Review.
-
Parenting stress and associated factors in healthcare workers after the second wave of COVID-19 in India: a two-center cross-sectional study.Front Psychiatry. 2023 Sep 12;14:1246540. doi: 10.3389/fpsyt.2023.1246540. eCollection 2023. Front Psychiatry. 2023. PMID: 37766928 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
