

Effect of Sodium-Glucose Cotransporter 2 Inhibitors for Heart Failure With Preserved Ejection Fraction: A Systematic Review and Meta-Analysis of Randomized Clinical Trials
- PMID: 35600478
- PMCID: PMC9116195
- DOI: 10.3389/fcvm.2022.875327
Effect of Sodium-Glucose Cotransporter 2 Inhibitors for Heart Failure With Preserved Ejection Fraction: A Systematic Review and Meta-Analysis of Randomized Clinical Trials
Abstract
Background: Heart failure with preserved ejection fraction (HFpEF) is associated with a high risk of mortality and frequent hospitalization. Sodium-glucose cotransporter 2 (SGLT2) inhibitors have favorable cardiovascular protective effect and could decrease the risk of mortality and hospitalization in patients with heart failure with reduced ejection fraction. However, the effect of SGLT2 inhibitors for HFpEF has not been well studied.
Purpose: The aim of this meta-analysis is to systematically assess the effects of SGLT2 inhibitors in patients with HFpEF.
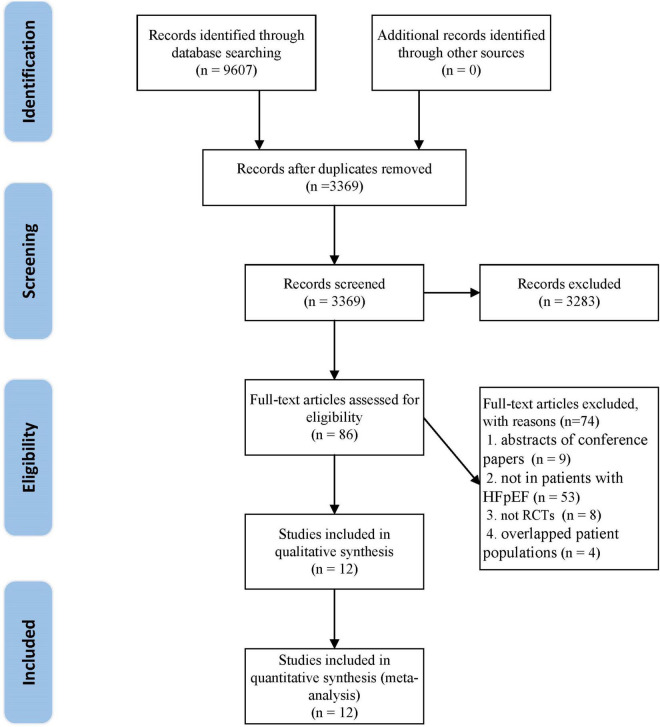
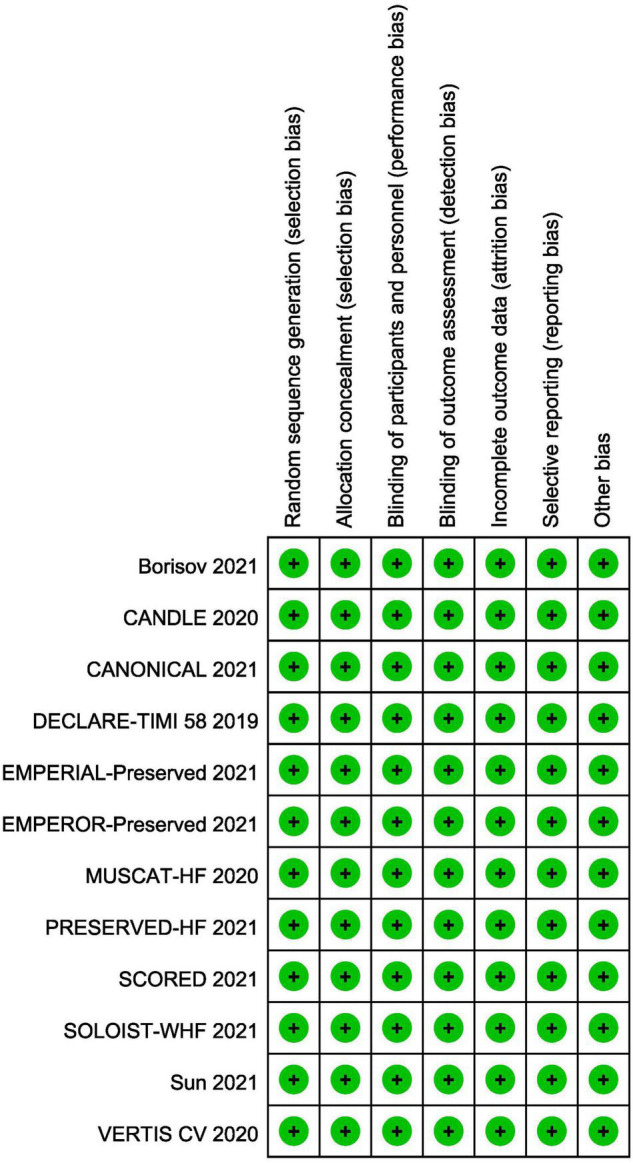
Methods: MEDLINE, EMBASE, Ovid, Cochrane Library, Chinese National Knowledge Infrastructure Database, VIP database, Chinese Biomedical Database, and Wanfang Database were searched from inception to November 2021 for randomized controlled trials (RCTs) of SGLT2 inhibitors for HFpEF. Risk bias was assessed for included studies according to Cochrane handbook. The primary outcome was the composite of first hospitalization for heart failure (HHF) or cardiovascular mortality. First HHF, cardiovascular mortality, total HHF, all-cause mortality, exercise capacity, ventricular diastolic function, and adverse events were considered as secondary endpoints. PROSPERO registration: CRD42021291122.
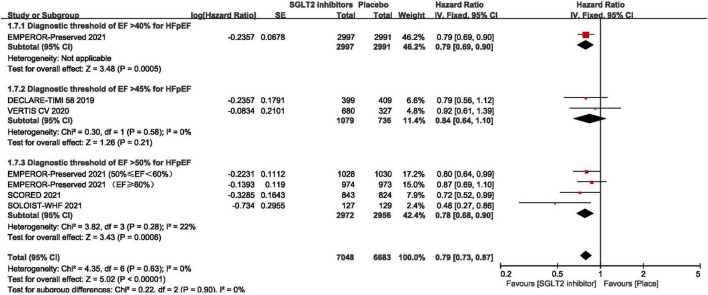
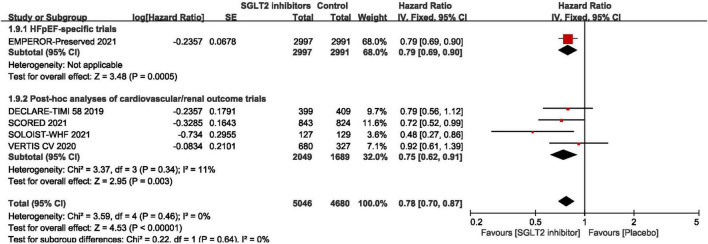
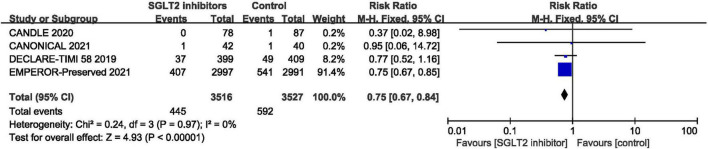
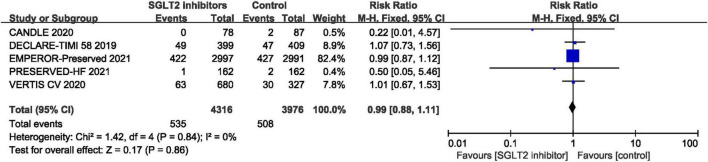
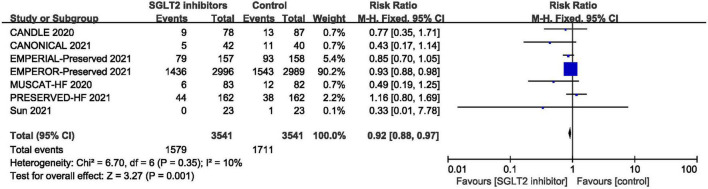
Results: A total of 12 RCTs including 10,883 patients with HFpEF (SGLT2 inhibitors group: 5,621; control group: 5,262) were included. All included RCTs were at low risk of bias. Meta-analysis showed that SGLT2 inhibitors significantly reduced the composite of first HHF or cardiovascular mortality (HR:0.78, 95% CI: [0.70, 0.87], P< 0.00001, I 2 = 0%), first HHF (HR:0.71, 95% CI: [0.62, 0.83], P < 0.00001, I 2 = 0%), total HHF (RR:0.75, 95% CI: [0.67, 0.84], P<0.00001, I 2 = 0%), E/e' (MD: -1.22, 95% CI: [-2.29, -0.15], P = 0.03, I 2 = 59%) and adverse events (RR:0.92, 95% CI: [0.88, 0.97], P = 0.001, I 2 = 0%). No statistical differences were found in terms of cardiovascular mortality, all-cause mortality, NT-proBNP, BNP and 6-min walk test distance.
Conclusion: SGLT2 inhibitors significantly improve cardiovascular outcomes with a lower risk of serious adverse events in patients with HFpEF. However, these findings require careful recommendation due to the small number of RCTs at present. More multi-center, randomized, double-blind, placebo-controlled trials are needed.
Systematic review registration: [https://www.crd.york.ac.Uk/prospero/], identifier [CRD42021291122].
Keywords: heart failure with preserved ejection fraction; meta-analysis; randomized controlled trials; sodium-glucose cotransporter 2 inhibitors; systematic review.
Copyright © 2022 Zhou, Peng, Li, Wang, Wang, Ding, Lin, Zhao, Pan and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021) 42:3599–726. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials