

Case Report: Juvenile Myelomonocytic Leukemia Underlying Ornithine Transcarbamylase Deficiency Safely Treated Using Hematopoietic Stem Cell Transplantation
- PMID: 35601422
- PMCID: PMC9120833
- DOI: 10.3389/fped.2022.898531
Case Report: Juvenile Myelomonocytic Leukemia Underlying Ornithine Transcarbamylase Deficiency Safely Treated Using Hematopoietic Stem Cell Transplantation
Abstract
Background: Juvenile myelomonocytic leukemia (JMML), which is predominantly found in infants, is a clonal abnormality of pluripotent hematopoietic stem cells and presents with the symptoms of both myeloproliferative tumors and myelodysplastic syndromes. Estimates have shown that ~20 cases of JMML occur annually in Japan. Ornithine transcarbamylase deficiency (OTCD), the most common among all urea cycle disorders (UCDs), occurs in 1 of 80,000 people in Japan.
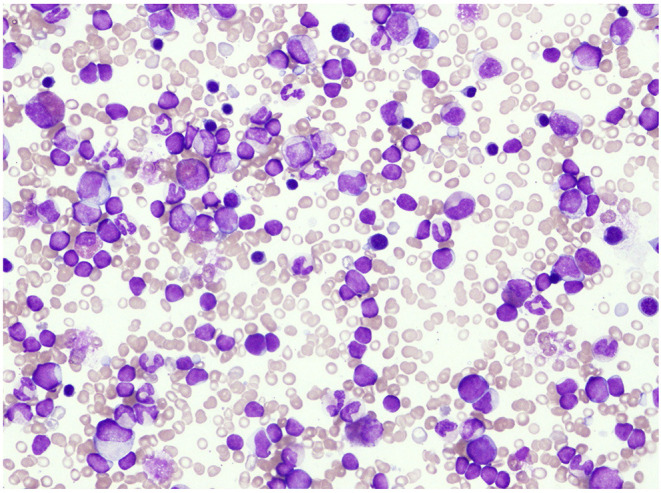
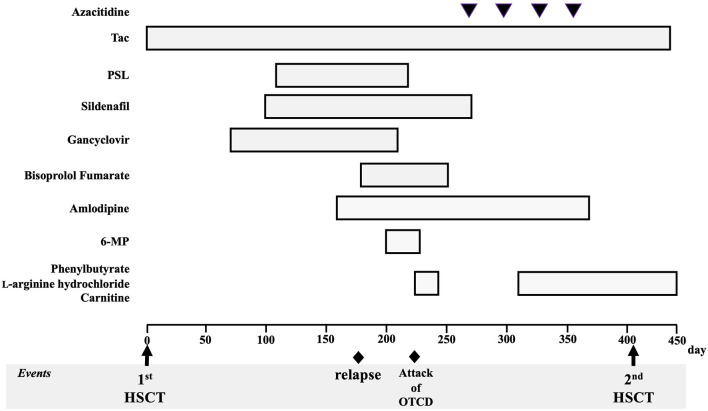
Case presentation: A 10-month-old infant who had fever, vomiting, and diarrhea for 2 days was referred to our hospital for the following abnormalities in blood tests: white blood cell count, 48,200/μL; hemoglobin, 9.0 g/dL; and platelet count, 135,000/μL. Bone marrow examination showed a nucleated cell count of 396,000/mm3 and blast cell count of 5.0%, as well as decreased mature granulocyte count and slightly myeloperoxidase stain-negative blasts but no monoclonal cell proliferation on May-Giemsa staining. Colony assay showed the proliferation of spontaneous colony and high sensitivity to granulocyte-macrophage colony-stimulating factor. Genetic analysis of peripheral blood mononuclear cells showed that the patient was positive for neuroblastoma RAS (NRAS) mutation. The patient was ultimately diagnosed with JMML. Approximately 170 days after his first hematopoietic stem cell transplantation (HSCT), the patient's JMML relapsed. Shortly after the recurrence, nausea, vomiting, hyperventilation, and decreased vitality were observed, followed by a decrease in the level of consciousness. The patient's ammonia level was 472 μmol/L. A test for seven different genetic mutations for the UCD showed the presence of c. 119G>A (amino acid change p. Arg40His). As such, late-onset OTCD was added to his diagnosis. Administration of sodium phenylacetate, l-arginine hydrochloride, and carnitine was continued following the diagnosis of OTCD, after which hyperammonemia was not observed. Regarding JMML relapse, HSCT was performed on day 405 after the first transplantation.
Conclusion: Hyperammonemia should be considered a differential diagnosis when unexplained and non-specific symptoms occur during the treatment of hematologic malignancies. Patients should be tested for UCD as a cause of hyperammonemia, and treatment for hyperammonemia should be continued until the cause is identified. The patient shows normal developmental progress, has an intact neurological status, and has not experienced another hyperammonemia attack. His JMML has remained in remission for over 3 years.
Keywords: chemotherapy; hematopoietic stem cell transplantation; hyperammonemia; juvenile myelomonocytic leukemia; ornithine transcarbamylase deficiency; urea cycle disorder.
Copyright © 2022 Eguchi, Kakiuchi, Nishi, Kojima-Ishii, Nishiyama, Koga and Matsuo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Niemeyer CM, Arico M, Basso G, Biondi A, Cantu Rajnoldi A, Creutzig U, et al. Chronic myelomonocytic leukemia in childhood: a retrospective analysis of 110 cases. European Working Group on myelodysplastic Syndromes in Childhood (EWOG-MDS). Blood. (1997) 89:3534–43 - PubMed
-
- Donovan K, Guzman N. Ornithine transcarbamylase deficiency. StatPearls, StatPearls Publishing LLC. (2022). Treasure Island (FL): StatPearls Publishing Copyright © 2022 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous