

Mechanisms of Immune Dysregulation in COVID-19 Are Different From SARS and MERS: A Perspective in Context of Kawasaki Disease and MIS-C
- PMID: 35601440
- PMCID: PMC9119432
- DOI: 10.3389/fped.2022.790273
Mechanisms of Immune Dysregulation in COVID-19 Are Different From SARS and MERS: A Perspective in Context of Kawasaki Disease and MIS-C
Abstract
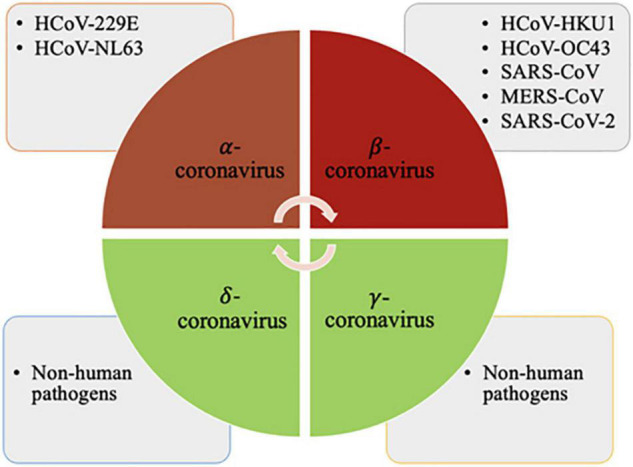
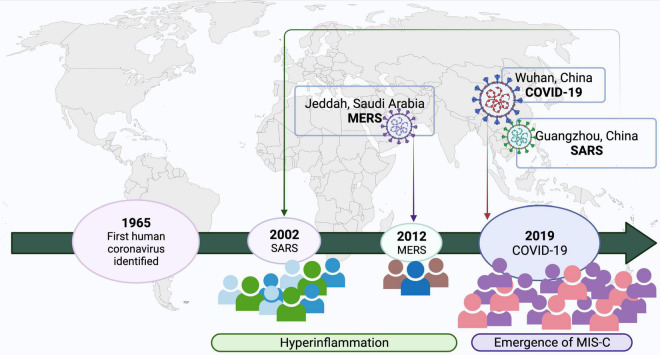
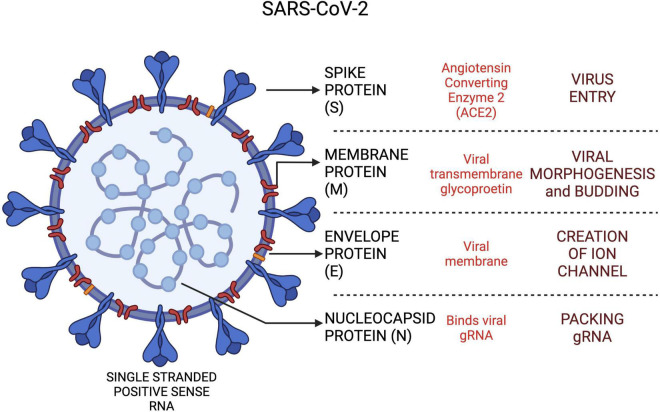
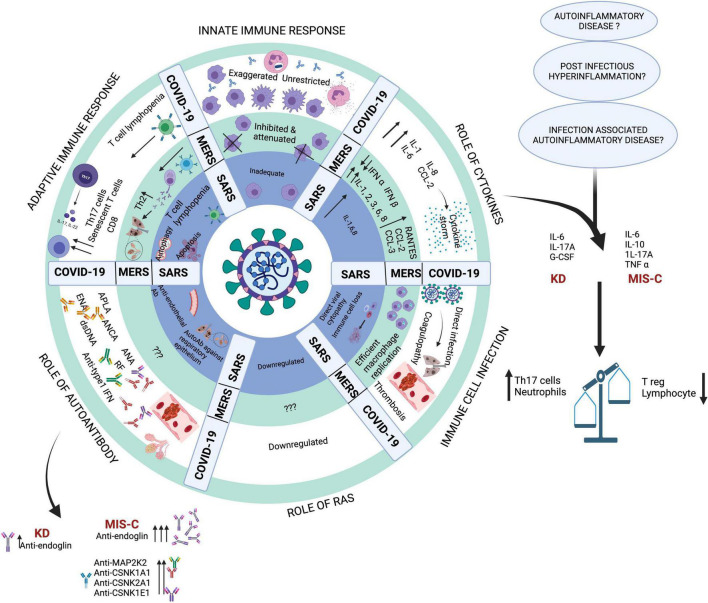
Coronaviruses have led to three major outbreaks to date-Severe Acute Respiratory Syndrome (SARS; 2002), Middle East Respiratory Syndrome (MERS; 2012) and the ongoing pandemic, Coronavirus Disease (COVID-19; 2019). Coronavirus infections are usually mild in children. However, a few children with MERS had presented with a severe phenotype in the acute phase resulting in progressive pneumonic changes with increasing oxygen dependency and acute respiratory distress requiring ventilatory support. A subset of children with a history of SARS-CoV-2 infection develops a multisystem hyper-inflammatory phenotype known as Multisystem Inflammatory Syndrome in Children (MIS-C). This syndrome occurs 4-6 weeks after infection with SARS-CoV-2 and has been reported more often from areas with high community transmission. Children with MIS-C present with high fever and often have involvement of cardiovascular, gastrointestinal and hematologic systems leading to multiorgan failure. This is accompanied by elevation of pro-inflammatory cytokines such as IL-6 and IL-10. MIS-C has several similarities with Kawasaki disease (KD) considering children with both conditions present with fever, rash, conjunctival injection, mucosal symptoms and swelling of hands and feet. For reasons that are still not clear, both KD and MIS-C were not reported during the SARS-CoV and MERS-CoV outbreaks. As SARS-CoV-2 differs from SARS-CoV by 19.5% and MERS by 50% in terms of sequence identity, differences in genomic and proteomic profiles may explain the varied disease immunopathology and host responses. Left untreated, MIS-C may lead to severe abdominal pain, ventricular dysfunction and shock. Immunological investigations reveal reduced numbers of follicular B cells, increased numbers of terminally differentiated CD4+T lymphocytes, and decreased IL-17A. There is still ambiguity about the clinical and immunologic risk factors that predispose some children to development of MIS-C while sparing others. Host-pathogen interactions in SARS, MERS and COVID-19 are likely to play a crucial role in the clinical phenotypes that manifest. This narrative review focuses on the immunological basis for development of MIS-C syndrome in the ongoing SARS-CoV-2 pandemic. To the best of our knowledge, these aspects have not been reviewed before.
Keywords: COVID-19; Kawasaki disease; MERS-CoV; MIS-C; SARS-CoV; SARS-CoV-2; immune dysregulation.
Copyright © 2022 Dhaliwal, Tyagi, Malhotra, Barman, Loganathan, Sharma, Sharma, Mondal, Rawat and Singh.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous