

Characterization of SARS-CoV-2 and host entry factors distribution in a COVID-19 autopsy series
- PMID: 35602214
- PMCID: PMC9053209
- DOI: 10.1038/s43856-021-00025-z
Characterization of SARS-CoV-2 and host entry factors distribution in a COVID-19 autopsy series
Abstract
Background: SARS-CoV-2 is a highly contagious virus that causes the disease COVID-19. We have recently reported that androgens regulate the expression of SARS-CoV-2 host entry factors ACE2 and TMPRSS2, and androgen receptor (AR) in lung epithelial cells. We also demonstrated that the transcriptional repression of the AR enhanceosome inhibited SARS-CoV-2 infection in vitro.
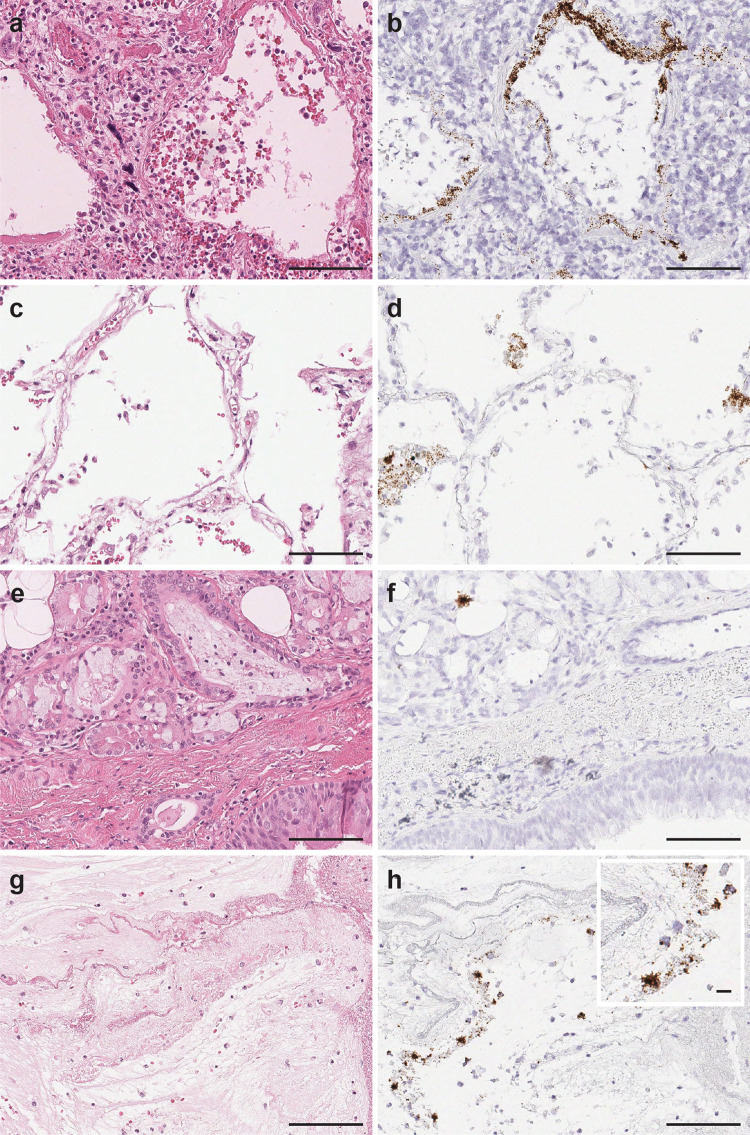
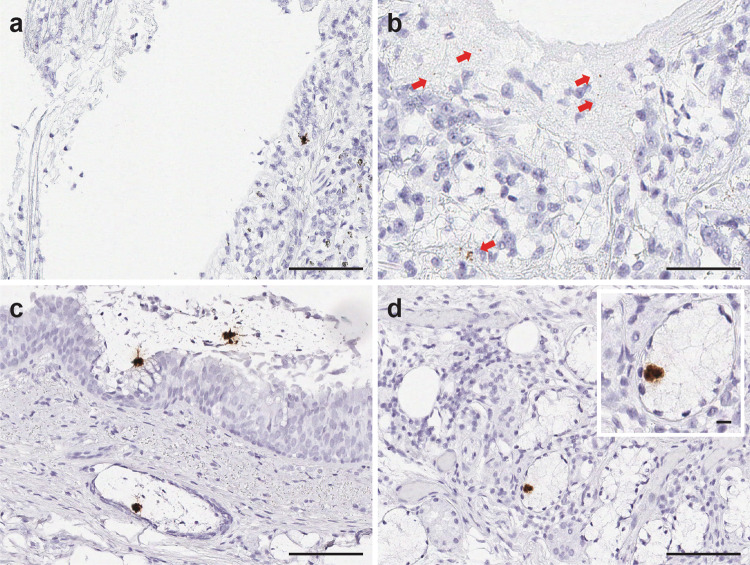
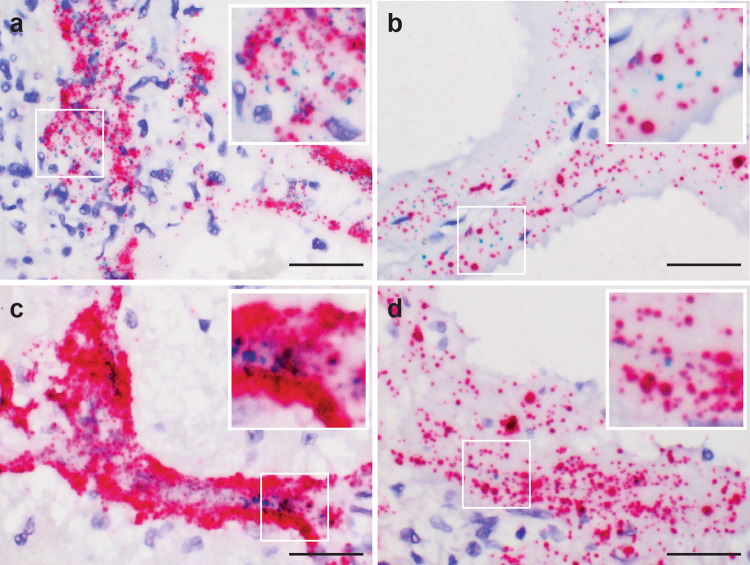
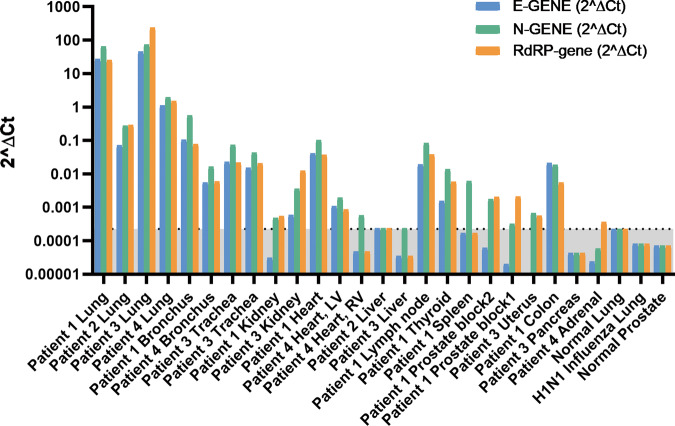
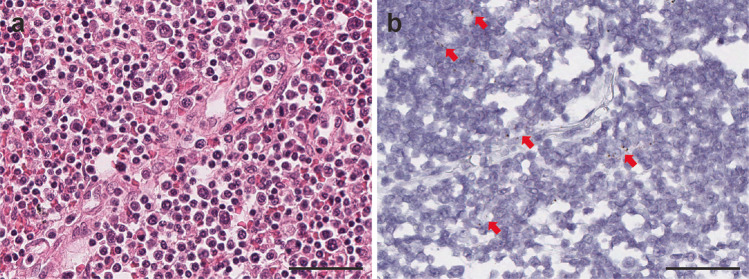
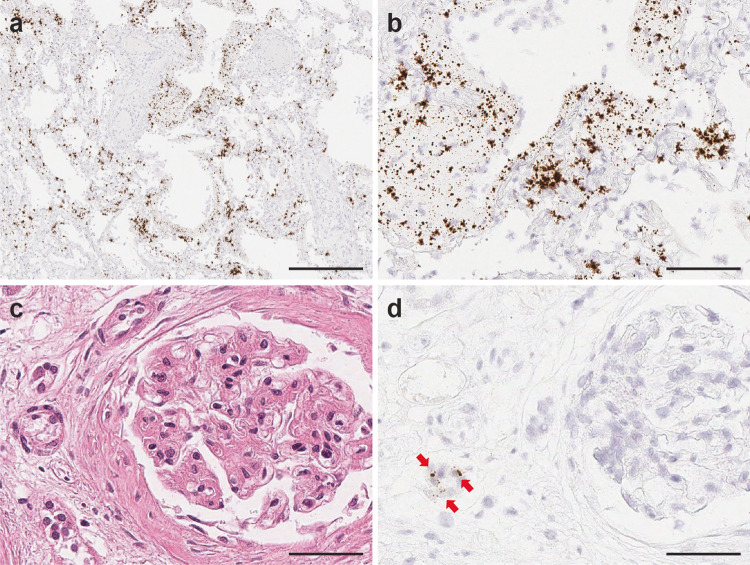
Methods: To better understand the various sites of SARS-CoV-2 infection, and presence of host entry factors, we extensively characterized the tissue distribution and localization of SARS-CoV-2 virus, viral replication, and host entry factors in various anatomical sites sampled via autopsy. We applied RNA in-situ-hybridization (RNA-ISH), immunohistochemistry (IHC) and quantitative reverse transcription polymerase chain reaction (qRT-PCR) approaches. We also assessed histopathological changes in SARS-CoV-2 infected tissues.
Results: We detect SARS-CoV-2 virus and viral replication in pulmonary tissues by RNA-ISH and IHC and a variety of non-pulmonary tissues including kidney, heart, liver, spleen, thyroid, lymph node, prostate, uterus, and colon by qRT-PCR. We observe heterogeneity in viral load and viral cytopathic effects among various organ systems, between individuals and within the same patient. In a patient with a history of kidney transplant and under immunosuppressant therapy, we observe an unusually high viral load in lung tissue by RNA-ISH, IHC and qRT-PCR. SARS-CoV-2 virus is also detected in this patent's kidney, liver and uterus. We find ACE2, TMPRSS2 and AR expression to overlap with the infection sites.
Conclusions: This study portrays the impact of dispersed SARS-CoV-2 infection in diverse organ systems, thereby facilitating avenues for systematic therapeutic approaches.
Keywords: Diagnostic markers; Gene expression analysis; Respiratory distress syndrome; Viral infection.
© The Author(s) 2021.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures
References
-
- WHO. WHO Transmission of SARS-CoV-2: implications for infection prevention precautions. Scientific brief https://www.who.int/news-room/commentaries/detail/transmission-of-sars-c.... (July 9 2020).
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
