

Development and multicenter validation of chest X-ray radiography interpretations based on natural language processing
- PMID: 35602222
- PMCID: PMC9053275
- DOI: 10.1038/s43856-021-00043-x
Development and multicenter validation of chest X-ray radiography interpretations based on natural language processing
Abstract
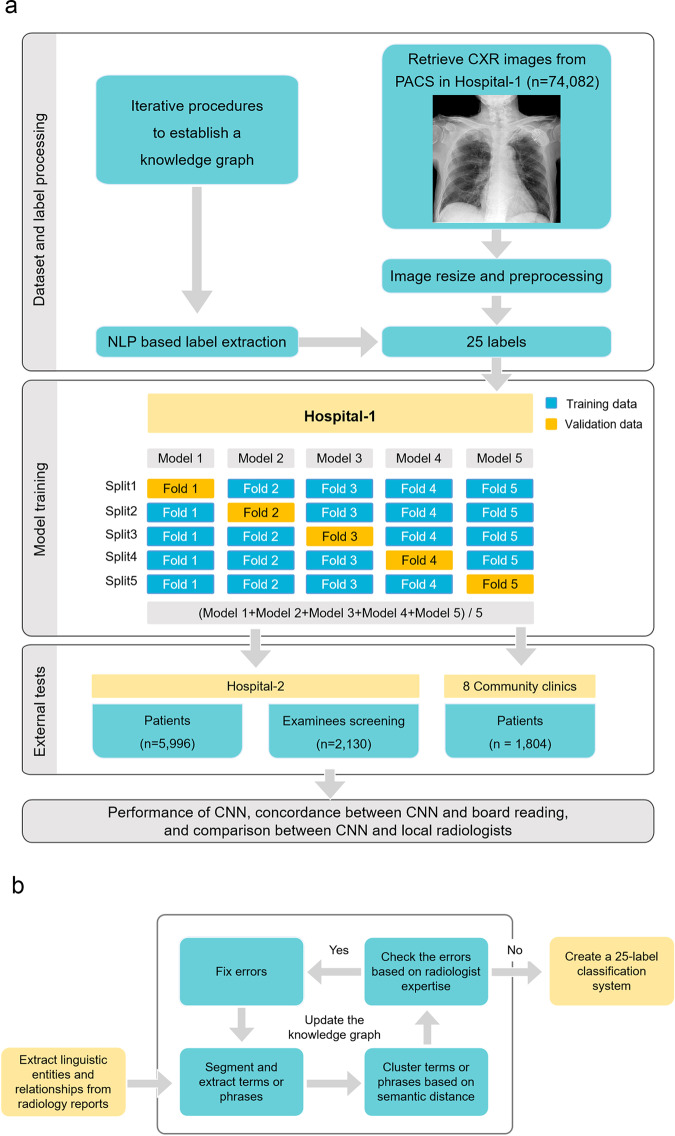
Background: Artificial intelligence can assist in interpreting chest X-ray radiography (CXR) data, but large datasets require efficient image annotation. The purpose of this study is to extract CXR labels from diagnostic reports based on natural language processing, train convolutional neural networks (CNNs), and evaluate the classification performance of CNN using CXR data from multiple centers.
Methods: We collected the CXR images and corresponding radiology reports of 74,082 subjects as the training dataset. The linguistic entities and relationships from unstructured radiology reports were extracted by the bidirectional encoder representations from transformers (BERT) model, and a knowledge graph was constructed to represent the association between image labels of abnormal signs and the report text of CXR. Then, a 25-label classification system were built to train and test the CNN models with weakly supervised labeling.
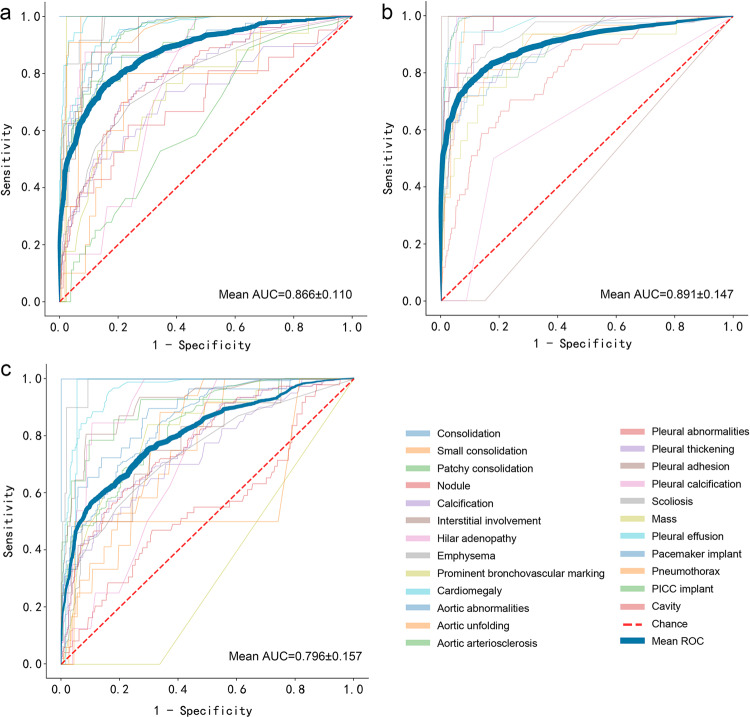
Results: In three external test cohorts of 5,996 symptomatic patients, 2,130 screening examinees, and 1,804 community clinic patients, the mean AUC of identifying 25 abnormal signs by CNN reaches 0.866 ± 0.110, 0.891 ± 0.147, and 0.796 ± 0.157, respectively. In symptomatic patients, CNN shows no significant difference with local radiologists in identifying 21 signs (p > 0.05), but is poorer for 4 signs (p < 0.05). In screening examinees, CNN shows no significant difference for 17 signs (p > 0.05), but is poorer at classifying nodules (p = 0.013). In community clinic patients, CNN shows no significant difference for 12 signs (p > 0.05), but performs better for 6 signs (p < 0.001).
Conclusion: We construct and validate an effective CXR interpretation system based on natural language processing.
Keywords: Computational biology and bioinformatics; Imaging.
© The Author(s) 2021.
Conflict of interest statement
Competing interestsThe authors declare the following competing interests: M.L., J.L. and X.C. are employees of Winning Health Technology Ltd., who have developed artificial intelligence methods and participated in drafting the technical part of this manuscript, but played no role in designing this study and analyzing the test data.
Figures



References
LinkOut - more resources
Full Text Sources
