

Effectiveness of Metacognitive Therapy in Patients With Depression and Comorbid Anxiety Symptoms: A Case Series From India
- PMID: 35602823
- PMCID: PMC9115621
- DOI: 10.7759/cureus.24229
Effectiveness of Metacognitive Therapy in Patients With Depression and Comorbid Anxiety Symptoms: A Case Series From India
Abstract
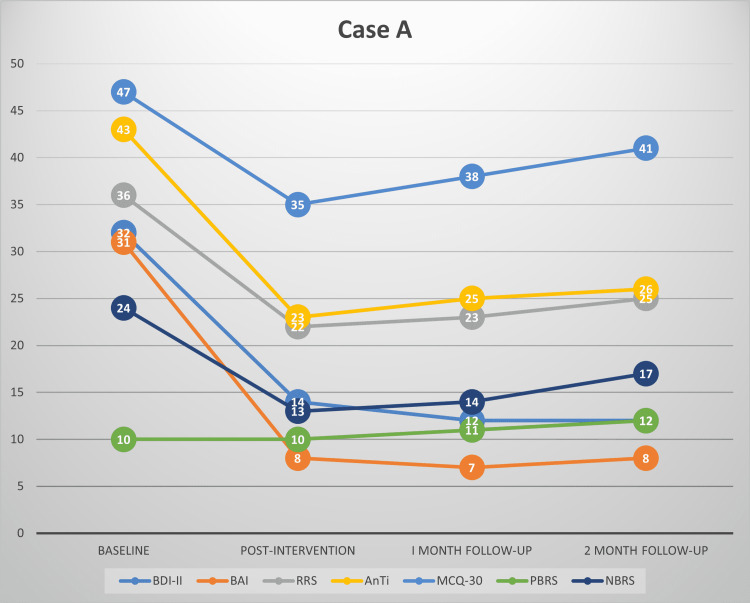
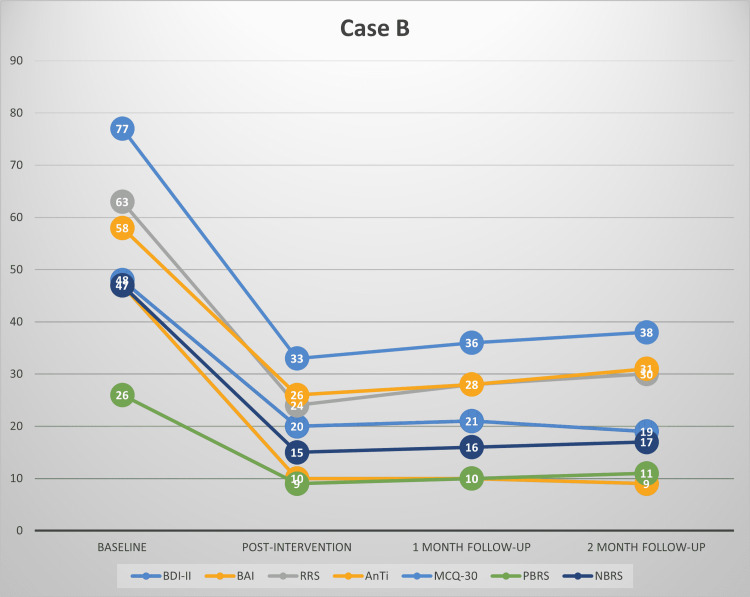
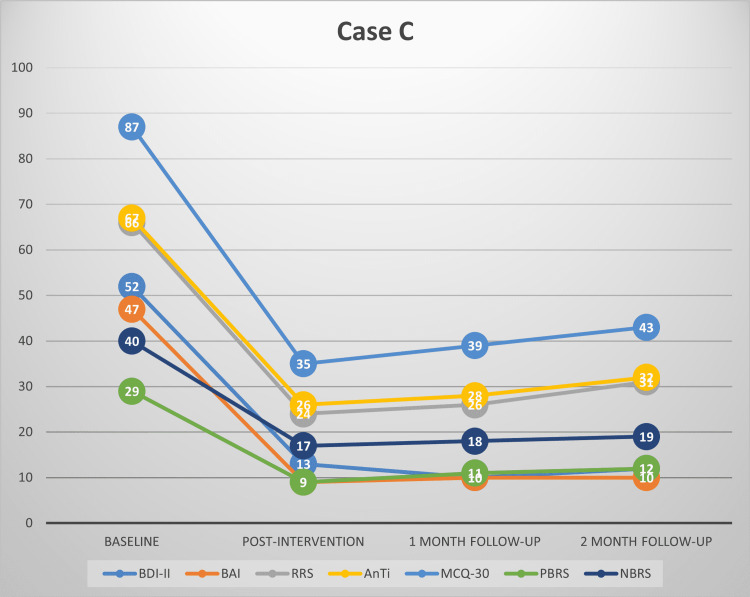
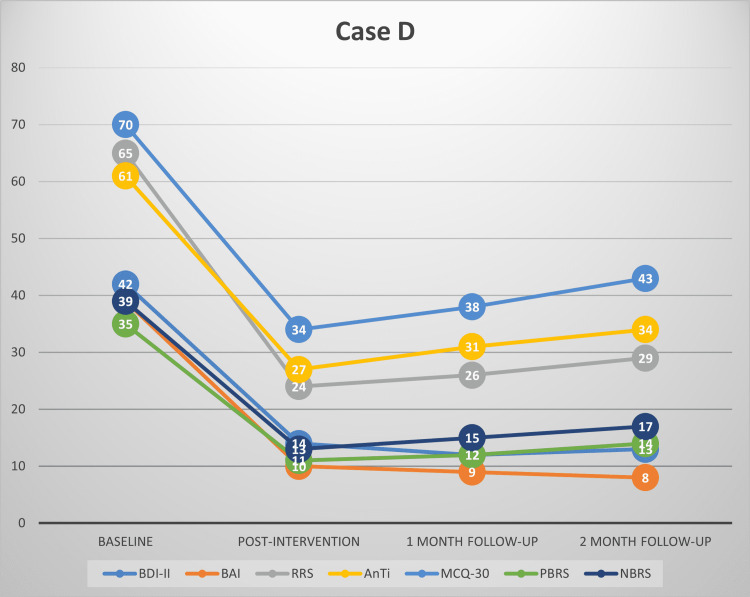
Metacognitive therapy (MCT) is a transdiagnostic intervention used to treat different psychiatric disorders. This intervention is based on the concept that persistent emotional distress is a consequence of a particular way of responding to negative thoughts and emotions. MCT for depression and anxiety aims at targeting rumination, worry, and the dysfunctional metacognitive beliefs underlying these thought processes. The purpose of this study was to explore MCT as a treatment for adult patients with depression (either major depressive disorder (MDD) or recurrent depressive disorder, dysthymia, or mixed anxiety depressive disorder) with comorbid anxiety symptoms. Four men diagnosed with depressive disorder with comorbid anxiety symptoms seeking treatment from the outpatient clinic of the Department of Psychiatry at the All India Institute of Medical Sciences, New Delhi, were recruited for the study. Each patient received 10 individual weekly sessions of MCT, lasting up to 1 hour each. Participants were assessed at baseline, post-intervention (right after completing MCT), and at one-month and two-month follow-ups. Primary outcome measures were a reduction in the severity of depression, anxiety, worry, and rumination. Secondary outcome measures were changes in dysfunctional metacognitive beliefs about worry and rumination. All outcomes were assessed via self-report using standardized questionnaires at baseline, post-intervention, one-month, and two-month follow-up. Data for all the outcome measures (at baseline, post-intervention, one month, and two-month follow-up) were plotted on a graph for visual examination. Additionally, we calculated clinically significant change (≥50% reduction in symptom severity and one other standardized criteria for clinically significant changes) for all the primary outcome measures across the above-mentioned four time points. All four men were single, well-educated, and had a mean age of 25.5±4.79 years. Their mean illness duration was 21±0.64 months. None of them had ever received any psychotherapy for their current illness. They had severe depressive and anxiety symptoms at baseline. Three participants had high scores on the rumination and worry scales. At post-intervention, all the participants had significant improvement on all the primary outcome measures, and they maintained their gains on follow-up assessments. Our study generated preliminary evidence supporting the effectiveness of MCT in treating depressive disorders with comorbid anxiety symptoms in the Indian context.
Keywords: anxiety; depression; dysfunctional metacognitive beliefs; metacognitive therapy; rumination; worry.
Copyright © 2022, Sharma et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Improving the effectiveness of psychological interventions for depression and anxiety in the cardiac rehabilitation pathway using group-based metacognitive therapy (PATHWAY Group MCT): study protocol for a randomised controlled trial.Trials. 2018 Apr 3;19(1):215. doi: 10.1186/s13063-018-2593-8. Trials. 2018. PMID: 29615092 Free PMC article.
-
Do metacognitive beliefs predict rumination and psychological distress independently of illness representations in adults with diabetes mellitus? A prospective mediation study.Br J Health Psychol. 2023 Sep;28(3):814-828. doi: 10.1111/bjhp.12655. Epub 2023 Mar 1. Br J Health Psychol. 2023. PMID: 36859760
-
Metacognitive Therapy for Emotional Distress in Adult Cancer Survivors: A Case Series.Cognit Ther Res. 2017;41(6):891-901. doi: 10.1007/s10608-017-9862-9. Epub 2017 May 29. Cognit Ther Res. 2017. PMID: 29104332 Free PMC article.
-
The Scope of Metacognitive Therapy in the Treatment of Psychiatric Disorders.Cureus. 2022 Mar 23;14(3):e23424. doi: 10.7759/cureus.23424. eCollection 2022 Mar. Cureus. 2022. PMID: 35475111 Free PMC article. Review.
-
[The powerlessness of thoughts – metacognitive therapy for children and adolescents].Z Kinder Jugendpsychiatr Psychother. 2016 Nov;44(6):423-431. doi: 10.1024/1422-4917/a000438. Epub 2016 Jun 13. Z Kinder Jugendpsychiatr Psychother. 2016. PMID: 27299518 Review. German.
References
-
- The epidemiology of comorbidity between depression, anxiety disorders and somatic diseases. Maier W, Falkai P. https://pubmed.ncbi.nlm.nih.gov/10471166/ Int Clin Psychopharmacol. 1999;14 Suppl 2:0–6. - PubMed
-
- Reexamining associations between mania, depression, anxiety and substance use disorders: results from a prospective national cohort. Olfson M, Mojtabai R, Merikangas KR, Compton WM, Wang S, Grant BF, Blanco C. Mol Psychiatry. 2017;22:235–241. - PubMed
-
- APA clinical practice guideline for the treatment of depression across three. [ Apr; 2022 ];Guideline Development Panel for the Treatment of Depressive Disorders. https://www.apa.org/depression-guideline 2019 505892019:1.
-
- Cognitive-behavioral analysis system of psychotherapy, drug, or their combination for persistent depressive disorder: personalizing the treatment choice using individual participant data network metaregression. Furukawa TA, Efthimiou O, Weitz ES, et al. Psychother Psychosom. 2018;87:140–153. - PubMed
Publication types
LinkOut - more resources
Full Text Sources