

Liver Stiffness by Transient Elastography Correlates With Degree of Portal Hypertension in Common Variable Immunodeficiency Patients With Nodular Regenerative Hyperplasia
- PMID: 35603209
- PMCID: PMC9121126
- DOI: 10.3389/fimmu.2022.864550
Liver Stiffness by Transient Elastography Correlates With Degree of Portal Hypertension in Common Variable Immunodeficiency Patients With Nodular Regenerative Hyperplasia
Abstract
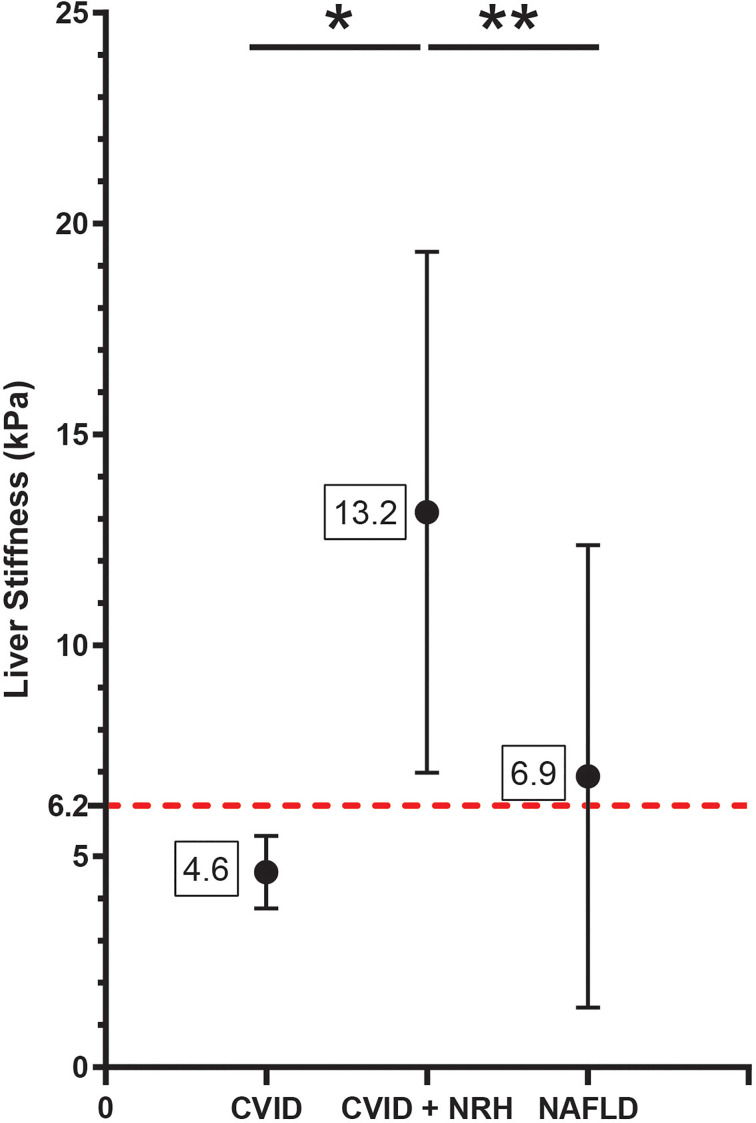
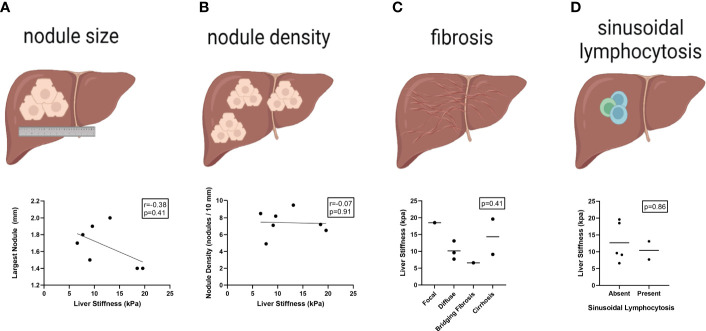
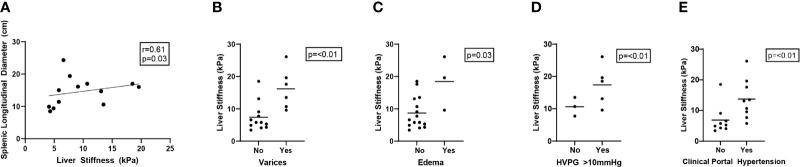
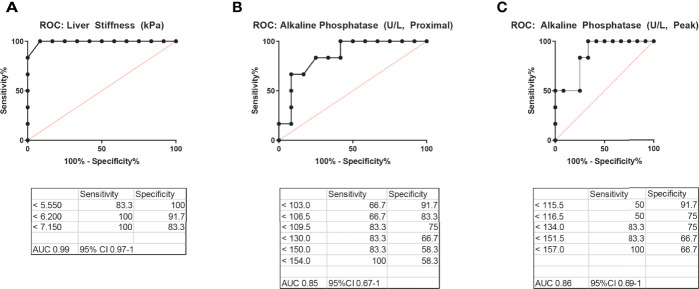
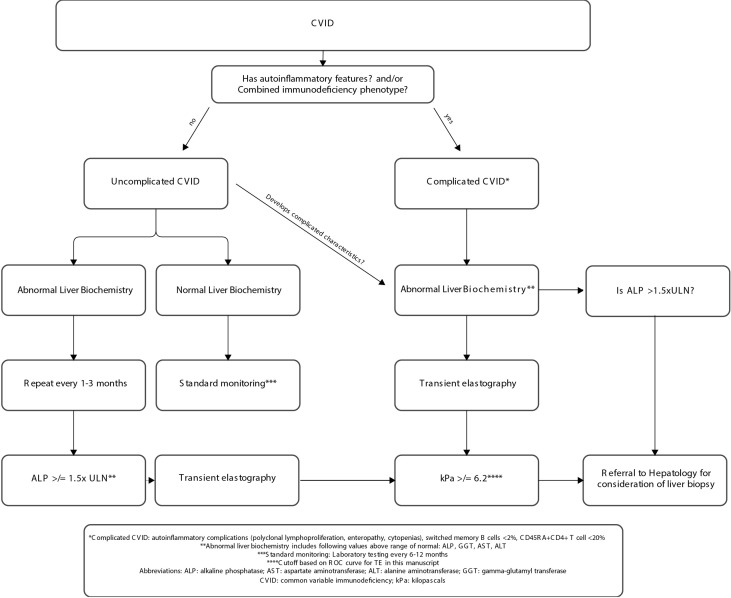
Nodular regenerative hyperplasia (NRH) is associated with high morbidity and mortality in patients with common variable immunodeficiency (CVID). While liver biopsy is the gold standard for NRH diagnosis, a non-invasive technique could facilitate early disease recognition, monitoring, and/or immune intervention. We performed a cross-sectional analysis of ultrasound-based transient elastography (TE) in patients with CVID to evaluate liver stiffness and compared this between patients with (N = 12) and without (N = 6) biopsy-proven NRH. Additionally, these data were compared to a cohort followed at our institution for non-alcoholic fatty liver disease (NAFLD) (N = 527), a disease for which TE has routine diagnostic use. Clinical and pathologic features of NRH were evaluated as correlates of liver stiffness, and receiver operating characteristic curves were used to define a liver stiffness cutoff with diagnostic utility for NRH among CVID patients. CVID patients with NRH had a more severe disease presentation compared to those without. This included increased autoinflammatory disease comorbidities, combined B-cell and T-cell dysfunction, and abnormal liver biochemistries (specifically an increased mean alkaline phosphatase level [proximal to TE, 250 vs. 100 U/L; p = 0.03; peak, 314 vs. 114 U/L; p = 0.02). Results of TE demonstrated a significantly elevated liver stiffness in CVID patients with NRH (mean 13.2 ± 6.2 kPa) as compared to both CVID patients without NRH (mean 4.6 ± 0.9 kPa) and non-CVID patients with NAFLD (mean 6.9 ± 5.5 kPa) (p < 0.01). No single or composite histopathologic feature of NRH correlated with liver stiffness including nodule size, nodule density, sinusoidal dilation, fibrosis, and/or lymphocytosis. In contrast, liver stiffness by TE was significantly correlated with clinical parameters of portal hypertension, including an elevated hepatic venous pressure gradient, an increased splenic longitudinal diameter, presence of varices, and presence of peripheral edema. A liver stiffness of greater than or equal to 6.2 kPa was a clinically significant cutoff for NRH in CVID patients. We propose that TE has diagnostic utility in CVID, particularly in the presence of immunophenotypic features such as combined B-cell and T-cell dysfunction, autoinflammatory comorbidities, and/or abnormal liver tests. Elevated liver stiffness by TE should raise suspicion for NRH in patients with CVID and prompt expedited evaluation by hepatology.
Keywords: common variable immunodeficiency (CVID); fibroscan©; liver biopsy; liver disease; nodular regenerative hyperplasia (NRH); transient elastography (TE).
Copyright © 2022 DiGiacomo, Shay, Crotty, Yang, Bloom, Corey, Barmettler and Farmer.
Conflict of interest statement
JF holds investigator-initiated grants from Bristol Myers Squibb and Pfizer with no direct relation to the work presented. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Portal hypertension in common variable immunodeficiency disorders - a single center analysis on clinical and immunological parameter in 196 patients.Front Immunol. 2023 Dec 20;14:1268207. doi: 10.3389/fimmu.2023.1268207. eCollection 2023. Front Immunol. 2023. PMID: 38187397 Free PMC article.
-
Common variable immunodeficiency disorder (CVID)-related liver disease: assessment of the main histological aspects using novel semiquantitative scoring systems, image analysis and correlation with clinical parameters of liver stiffness and portal hypertension.J Clin Pathol. 2024 Sep 19;77(10):709-716. doi: 10.1136/jcp-2023-208977. J Clin Pathol. 2024. PMID: 37553247
-
[Nodular regenerative hyperplasia associated with common variable immunodeficiency and other comorbidities].Med Clin (Barc). 2016 Mar 18;146(6):263-6. doi: 10.1016/j.medcli.2015.11.008. Epub 2015 Dec 23. Med Clin (Barc). 2016. PMID: 26723943 Spanish.
-
Management of liver disease and portal hypertension in common variable immunodeficiency (CVID).JHEP Rep. 2023 Aug 13;5(11):100882. doi: 10.1016/j.jhepr.2023.100882. eCollection 2023 Nov. JHEP Rep. 2023. PMID: 37869072 Free PMC article. Review.
-
A Meta-analysis for the Diagnostic Performance of Transient Elastography for Clinically Significant Portal Hypertension.Ultrasound Med Biol. 2017 Jan;43(1):59-68. doi: 10.1016/j.ultrasmedbio.2016.07.025. Epub 2016 Oct 15. Ultrasound Med Biol. 2017. PMID: 27751595 Review.
Cited by
-
Common variable immunodeficiency disorder-related liver disease is common and results in portal hypertension and an increased risk of death.Hepatol Commun. 2023 Dec 15;8(1):e0322. doi: 10.1097/HC9.0000000000000322. eCollection 2024 Jan 1. Hepatol Commun. 2023. PMID: 38099861 Free PMC article.
-
A rare differential diagnosis of inflammatory bowel disease in a young male patient; a challenging case report.Gastroenterol Hepatol Bed Bench. 2024;17(2):206-211. doi: 10.22037/ghfbb.v17i2.2898. Gastroenterol Hepatol Bed Bench. 2024. PMID: 38994511 Free PMC article.
-
Portal hypertension in common variable immunodeficiency disorders - a single center analysis on clinical and immunological parameter in 196 patients.Front Immunol. 2023 Dec 20;14:1268207. doi: 10.3389/fimmu.2023.1268207. eCollection 2023. Front Immunol. 2023. PMID: 38187397 Free PMC article.
References
-
- Bonilla FA, Barlan I, Chapel H, Costa-Carvalho BT, Cunningham-Rundles C, de la Morena MT, et al. . International Consensus Document (ICON): Common Variable Immunodeficiency Disorders. In: Journal of Allergy and Clinical Immunology: In Practice, vol. 4. Milwaukee, WI: American Academy of Allergy, Asthma and Immunology; (2016). p. 38–59. doi: 10.1016/j.jaip.2015.07.025 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical