

A rapid antibody screening haemagglutination test for predicting immunity to SARS-CoV-2 variants of concern
- PMID: 35603265
- PMCID: PMC9053181
- DOI: 10.1038/s43856-022-00091-x
A rapid antibody screening haemagglutination test for predicting immunity to SARS-CoV-2 variants of concern
Abstract
Background: Evaluation of susceptibility to emerging SARS-CoV-2 variants of concern (VOC) requires rapid screening tests for neutralising antibodies which provide protection.
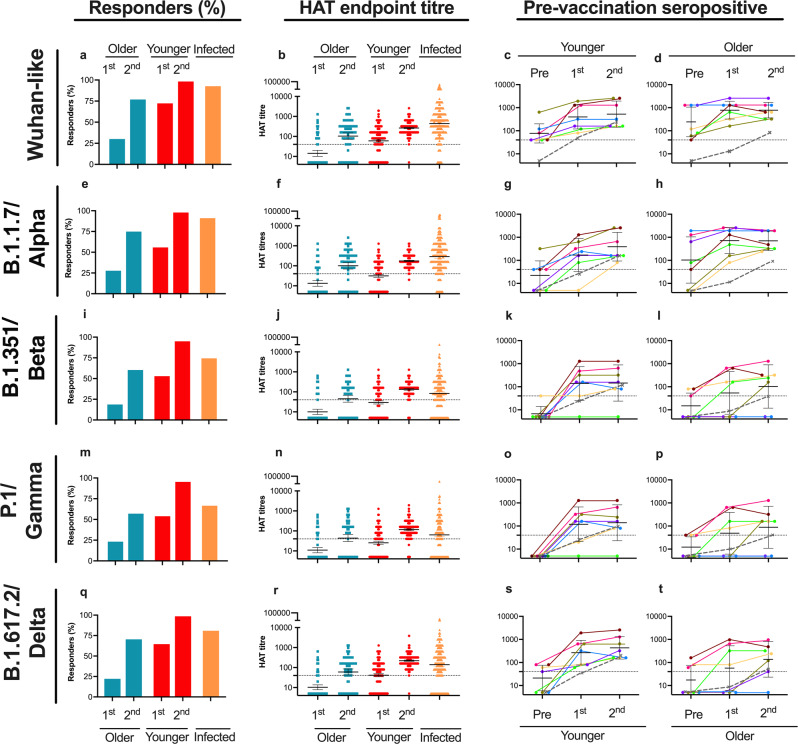
Methods: Firstly, we developed a receptor-binding domain-specific haemagglutination test (HAT) to Wuhan and VOC (alpha, beta, gamma and delta) and compared to pseudotype, microneutralisation and virus neutralisation assays in 835 convalescent sera. Secondly, we investigated the antibody response using the HAT after two doses of mRNA (BNT162b2) vaccination. Sera were collected at baseline, three weeks after the first and second vaccinations from older (80-99 years, n = 89) and younger adults (23-77 years, n = 310) and compared to convalescent sera from naturally infected individuals (1-89 years, n = 307).
Results: Here we show that HAT antibodies highly correlated with neutralising antibodies (R = 0.72-0.88) in convalescent sera. Home-dwelling older individuals have significantly lower antibodies to the Wuhan strain after one and two doses of BNT162b2 vaccine than younger adult vaccinees and naturally infected individuals. Moverover, a second vaccine dose boosts and broadens the antibody repertoire to VOC in naïve, not previously infected older and younger adults. Most (72-76%) older adults respond after two vaccinations to alpha and delta, but only 58-62% to beta and gamma, compared to 96-97% of younger vaccinees and 68-76% of infected individuals. Previously infected older individuals have, similarly to younger adults, high antibody titres after one vaccination.
Conclusions: Overall, HAT provides a surrogate marker for neutralising antibodies, which can be used as a simple inexpensive, rapid test. HAT can be rapidly adaptable to emerging VOC for large-scale evaluation of potentially decreasing vaccine effectiveness.
Keywords: Predictive markers; RNA vaccines; Viral infection.
© The Author(s) 2022.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures


References
LinkOut - more resources
Full Text Sources
Miscellaneous
