

German federal-state-wide seroprevalence study of 1st SARS-CoV-2 pandemic wave shows importance of long-term antibody test performance
- PMID: 35603305
- PMCID: PMC9117207
- DOI: 10.1038/s43856-022-00100-z
German federal-state-wide seroprevalence study of 1st SARS-CoV-2 pandemic wave shows importance of long-term antibody test performance
Abstract
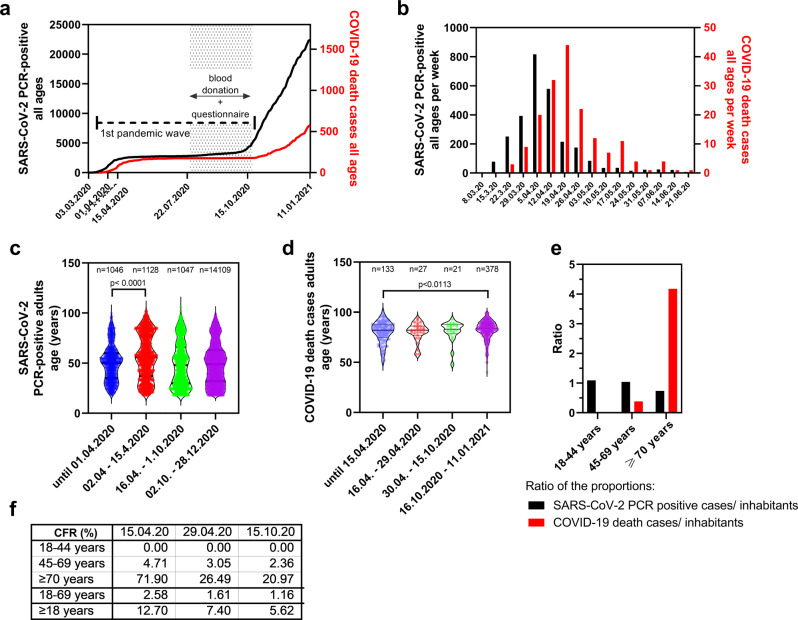
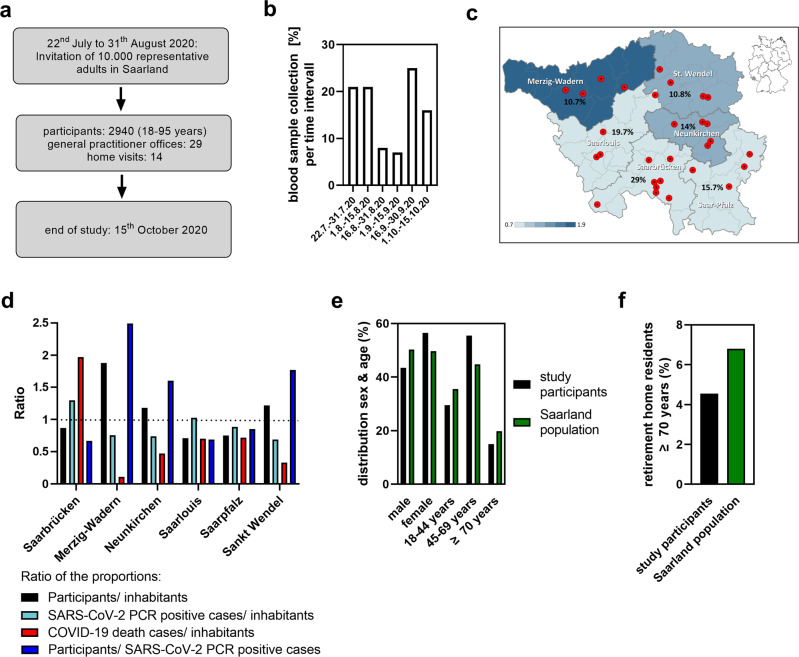
Background: Reliable data on the adult SARS-CoV-2 infection fatality rate in Germany are still scarce. We performed a federal state-wide cross-sectional seroprevalence study named SaarCoPS, that is representative for the adult population including elderly individuals and nursing home residents in the Saarland.
Methods: Serum was collected from 2940 adults via stationary or mobile teams during the 1st pandemic wave steady state period. We selected an antibody test system with maximal specificity, also excluding seroreversion effects due to a high longitudinal test performance. For the calculations of infection and fatality rates, we accounted for the delays of seroconversion and death after infection.
Results: Using a highly specific total antibody test detecting anti-SARS-CoV-2 responses over more than 180 days, we estimate an adult infection rate of 1.02% (95% CI: [0.64; 1.44]), an underreporting rate of 2.68-fold (95% CI: [1.68; 3.79]) and infection fatality rates of 2.09% (95% CI: (1.48; 3.32]) or 0.36% (95% CI: [0.25; 0.59]) in all adults including elderly individuals, or adults younger than 70 years, respectively.
Conclusion: The study highlights the importance of study design and test performance for seroprevalence studies, particularly when seroprevalences are low. Our results provide a valuable baseline for evaluation of future pandemic dynamics and impact of public health measures on virus spread and human health in comparison to neighbouring countries such as Luxembourg or France.
Keywords: Population screening; Viral infection.
© The Author(s) 2022.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures




References
LinkOut - more resources
Full Text Sources
Miscellaneous
