

Sex differences in efficacy of pharmacological therapies in heart failure with reduced ejection fraction: a meta-analysis
- PMID: 35603531
- PMCID: PMC9288771
- DOI: 10.1002/ehf2.13974
Sex differences in efficacy of pharmacological therapies in heart failure with reduced ejection fraction: a meta-analysis
Abstract
Aims: Recent studies have suggested potential sex differences in treatment response to pharmacological therapies in heart failure (HF). We performed a systematic review and meta-analysis of studies comparing treatment effects between men and women with HF and reduced ejection fraction (HFrEF) using established guideline-directed medical therapy and other emerging pharmacological treatments.
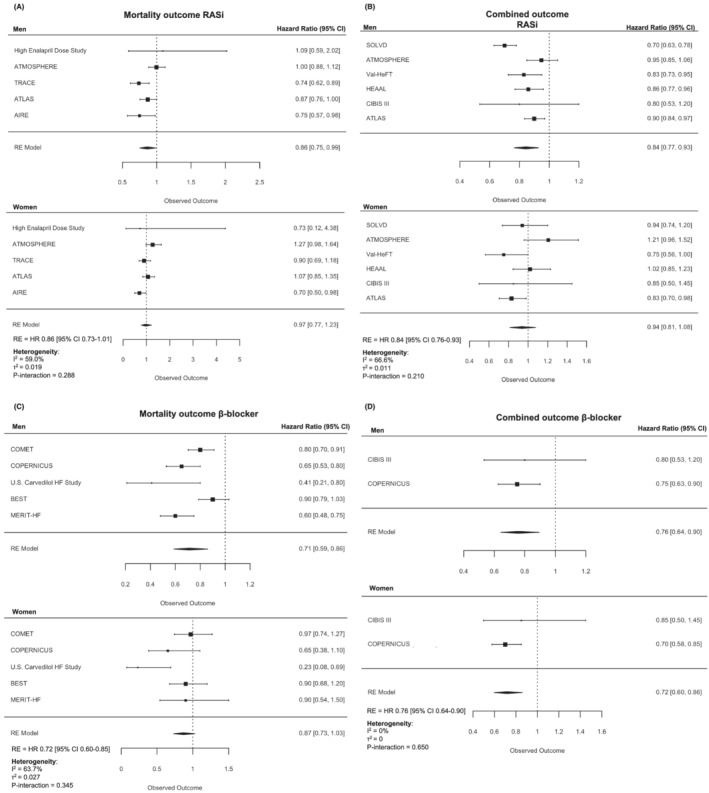
Methods and results: Systematic search was performed on PubMed, Embase, and Cochrane Library for randomized controlled trials published in 1990-2021. Outcomes were all-cause mortality and combined outcome of all-cause mortality and/or hospitalization for HF. Of 618 articles identified, 25 articles and 100 213 patients (mean age 62 ± 1.7 years, women 23.1%, mean left ventricular ejection fraction 26.6 ± 1.3%) were included in the systematic review and meta-analysis. For the outcome of all-cause mortality, there was no evidence of treatment heterogeneity by sex for renin-angiotensin system inhibitors (RASi) [hazard ratio (HR) 0.86 (95% confidence interval 0.75-0.99) in men; HR 0.97 (0.77-1.23) in women; Pinteraction = 0.288], or for beta-blockers (BB) [HR 0.71 (0.59-0.86) in men; HR 0.87 (0.73-1.03) in women; Pinteraction = 0.345]. Similarly, for the composite outcome of death or HF hospitalization, there was no evidence of treatment heterogeneity by sex for RASi [HR 0.84 (0.77-0.93) in men; HR 0.94 (0.81-1.08) in women; Pinteraction = 0.210] or BB [HR 0.76 (0.64-0.90) in men; HR 0.72 (0.60-0.86) in women; Pinteraction = 0.650]. Results for mineralocorticoid receptor antagonists (MRA) and sodium-glucose cotransporter-2 inhibitors (SGLT2i) from previously published meta-analyses were included in the review. For the combined outcome of cardiovascular death or HF hospitalization, no significant interaction for sex was observed for MRA (Pinteraction = 0.78) or SGLT2i (Pinteraction = 0.37). Results for emerging pharmacological treatments, such as soluble guanylate cyclase stimulators and cardiac myosin activators, were included in the review and showed consistent treatment effects between men and women.
Conclusions: Our meta-analysis showed no differences between sex in treatment effect for BB and RASi. Review on previously published trials for MRA, SGLT2i, and emerging therapies presented consistent treatment effects between men and women.
Keywords: Guideline-directed medical therapy; Heart failure with reduced ejection fraction; Pharmacology; Sex differences.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
The authors declared no conflict of interest relevant to the present work. C.S.L. is supported by a Clinician Scientist Award from the National Medical Research Council of Singapore; has received research support from Boston Scientific, Bayer, Roche Diagnostics, AstraZeneca, Medtronic, and Vifor Pharma; has served as consultant or on the Advisory Board/Steering Committee/Executive Committee for Boston Scientific, Bayer, Roche Diagnostics, AstraZeneca, Medtronic, Vifor Pharma, Novartis, Amgen, Merck, Janssen Research & Development LLC, Menarini, Boehringer Ingelheim, Novo Nordisk, Abbott Diagnostics, Corvia, Stealth BioTherapeutics, JanaCare, Biofourmis, Darma, Applied Therapeutics, MyoKardia, Cytokinetics, WebMD Global LLC, Radcliffe Group Ltd and Corpus; and serves as co‐founder & non‐executive director of eKo.ai.
Figures
References
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo‐Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray J, Mebazaa A, Mindham R, Muneretto C, Francesco Piepoli M, Price S, Rosano GMC, Ruschitzka F, Kathrine Skibelund A, ESC Scientific Document Group . 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2021; 42: 3599–3726. - PubMed
-
- Writing Committee , Maddox TM, Januzzi JL Jr, Allen LA, Breathett K, Butler J, Davis LL, Fonarow GC, Ibrahim NE, Lindenfeld J, Masoudi FA, Motiwala SR, Oliveros E, Patterson JH, Walsh MN, Wasserman A, Yancy CW, Youmans QR. 2021 Update to the 2017 ACC expert consensus decision pathway for optimization of heart failure treatment: answers to 10 pivotal issues about heart failure with reduced ejection fraction: a report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2021; 77: 772–810. - PubMed
-
- Teerlink JR, Diaz R, Felker GM, McMurray JJV, Metra M, Solomon SD, Adams KF, Anand I, Arias‐Mendoza A, Biering‐Sørensen T, Böhm M, Bonderman D, Cleland JGF, Corbalan R, Crespo‐Leiro MG, Dahlström U, Echeverria LE, Fang JC, Filippatos G, Fonseca C, Goncalvesova E, Goudev AR, Howlett JG, Lanfear DE, Li J, Lund M, Macdonald P, Mareev V, Momomura SI, O'Meara E, Parkhomenko A, Ponikowski P, Ramires FJA, Serpytis P, Sliwa K, Spinar J, Suter TM, Tomcsanyi J, Vandekerckhove H, Vinereanu D, Voors AA, Yilmaz MB, Zannad F, Sharpsten L, Legg JC, Varin C, Honarpour N, Abbasi SA, Malik FI, Kurtz CE, GALACTIC‐HF Investigators . Cardiac myosin activation with omecamtiv mecarbil in systolic heart failure. N Engl J Med. 2021; 384: 105–116. - PubMed
-
- Armstrong PW, Pieske B, Anstrom KJ, Ezekowitz J, Hernandez AF, Butler J, Lam CSP, Ponikowski P, Voors AA, Jia G, McNulty SE, Patel MJ, Roessig L, Koglin J, O'Connor CM. Vericiguat in patients with heart failure and reduced ejection fraction. N Engl J Med. 2020; 382: 1883–1893. - PubMed
-
- Whitley H, Lindsey W. Sex‐based differences in drug activity. Am Fam Physician. 2009; 80: 1254–1258. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
