

Revision arthroplasty with megaprosthesis after Girdlestone procedure for periprosthetic joint infection as an option in massive acetabular and femoral bone defects
- PMID: 35604274
- PMCID: PMC9437688
- DOI: 10.23750/abm.v92iS3.12160
Revision arthroplasty with megaprosthesis after Girdlestone procedure for periprosthetic joint infection as an option in massive acetabular and femoral bone defects
Abstract
Background and aim: To evaluate the clinical outcomes of patients treated with Girdlestone procedure (GP) or excision arthroplasty (EA) for periprosthetic infection with massive bone defects and undergoing revision arthroplasty.
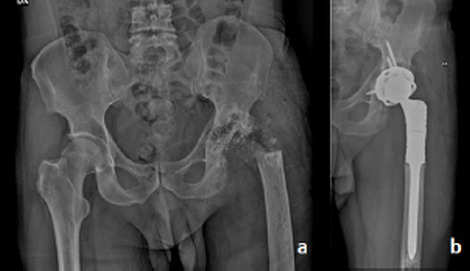
Methods: All patients treated with EA or GP for hip periprosthetic infection between 2014 and 2017 and sustaining revision arthroplasty (RA) were included in the study. Patients with less than 24 months of follow-up or less than 12 months between GP or EA and RA were excluded. Any sign of implant mobilization or periprosthetic fracture was assessed through X-ray. Patients were evaluated with D'aubignè-Postel hip score before RA and at the last follow-up. Mann-Whitney U test was used to assess differences between pre-RA surgery and last follow-up. P value was set as <0.05.
Results: Twelve patients meet the inclusion criteria (mean follow-up 58+/-9.72 months). No radiographic sign of implant mobilization or periprosthetic fracture was reported. A significant difference was found for each parameter of the D'Aubigne-Postel score (p < 0.0001); none of the patients reached more than fair results in the absolute hip score. The difference between pre and post-operative global status showed a fair improvement. A significant difference was found for leg length discrepancy between pre and post RA (p<0.0001).
Conclusions: Conversion from EA or GP to RA in patients suffering from massive acetabular and femur defects is challenging; conversion procedure is able to reduce patients' disability and to improve walking ability. (www.actabiomedica.it).
Conflict of interest statement
Each author declares that he has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
Figures

Similar articles
-
The Influence of Spacer Design on the Rate of Complications in Two-Stage Revision Hip Arthroplasty.J Arthroplasty. 2019 Jun;34(6):1201-1206. doi: 10.1016/j.arth.2019.02.012. Epub 2019 Feb 15. J Arthroplasty. 2019. PMID: 30879874
-
[The Role of a Modular Universal Tumour and Revision System (MUTARS®) in Lower Limb Endoprosthetic Revision Surgery - Outcome Analysis of 25 Patients].Z Orthop Unfall. 2017 Feb;155(1):61-66. doi: 10.1055/s-0042-114704. Epub 2016 Sep 15. Z Orthop Unfall. 2017. PMID: 27632667 German.
-
Periprosthetic femoral fractures after total hip arthroplasty: An algorithm of treatment.Injury. 2019 Jul;50 Suppl 2:S45-S51. doi: 10.1016/j.injury.2019.01.044. Epub 2019 Feb 2. Injury. 2019. PMID: 30765184
-
[Periprosthetic fractures of the acetabulum: revision endoprosthetics].Chirurg. 2020 Oct;91(10):823-832. doi: 10.1007/s00104-020-01240-5. Chirurg. 2020. PMID: 32691082 Review. German.
-
Management of Periprosthetic Acetabular Fractures: A Critical Analysis and Review of the Literature.JBJS Rev. 2022 Aug 11;10(8). doi: 10.2106/JBJS.RVW.22.00073. eCollection 2022 Aug 1. JBJS Rev. 2022. PMID: 35959937 Review.
Cited by
-
Extracapsular femoral neck fractures treated with total hip arthroplasty: identification of a population with better outcomes.Orthop Rev (Pavia). 2022 Oct 13;14(6):38576. doi: 10.52965/001c.38576. eCollection 2022. Orthop Rev (Pavia). 2022. PMID: 36267219 Free PMC article.
-
Subtrochanteric femoral fractures: A case series of 194 patients treated with long and short intramedullary nails.Orthop Rev (Pavia). 2022 Oct 13;14(6):38613. doi: 10.52965/001c.38613. eCollection 2022. Orthop Rev (Pavia). 2022. PMID: 36267212 Free PMC article.
-
WHICH PROBLEMATICS IN THA AFTER ACETABULAR FRACTURES: EXPERIENCE OF 38 CASES.Orthop Rev (Pavia). 2022 Oct 13;14(6):38611. doi: 10.52965/001c.38611. eCollection 2022. Orthop Rev (Pavia). 2022. PMID: 36267215 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
