

Enduring undetectable MRD and updated outcomes in relapsed/refractory CLL after fixed-duration venetoclax-rituximab
- PMID: 35605176
- PMCID: PMC9412011
- DOI: 10.1182/blood.2021015014
Enduring undetectable MRD and updated outcomes in relapsed/refractory CLL after fixed-duration venetoclax-rituximab
Abstract
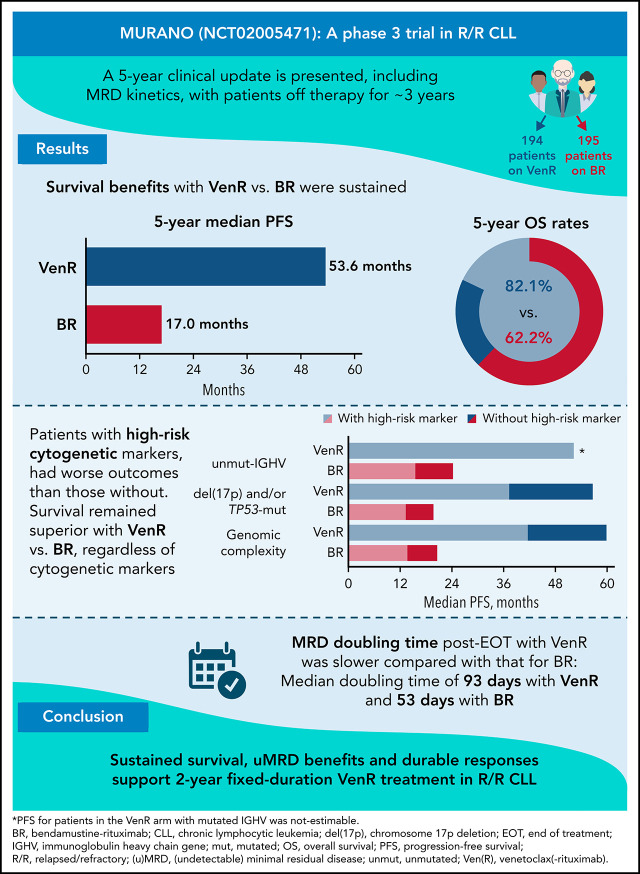
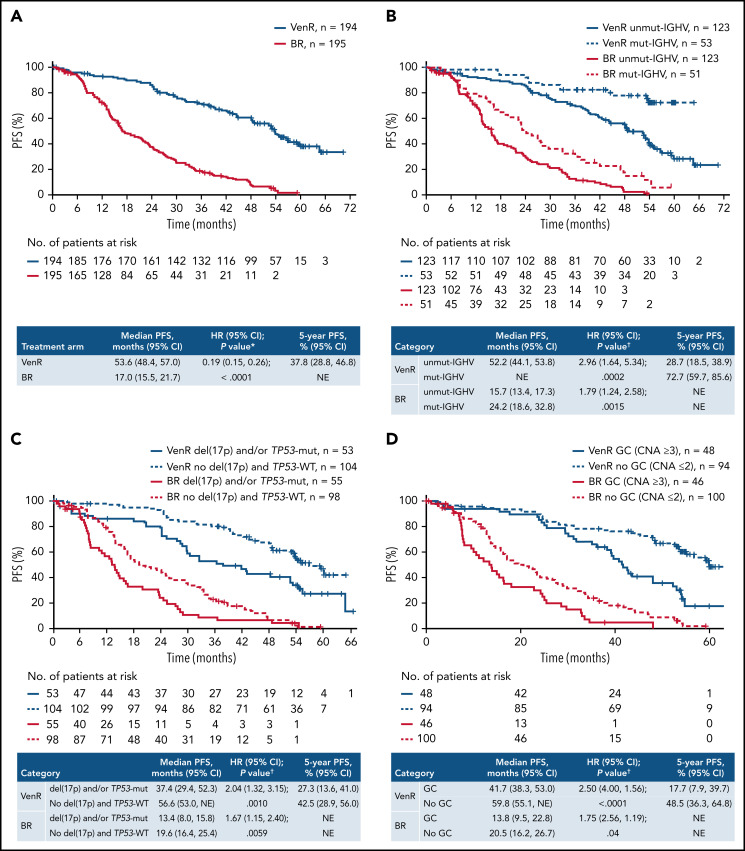
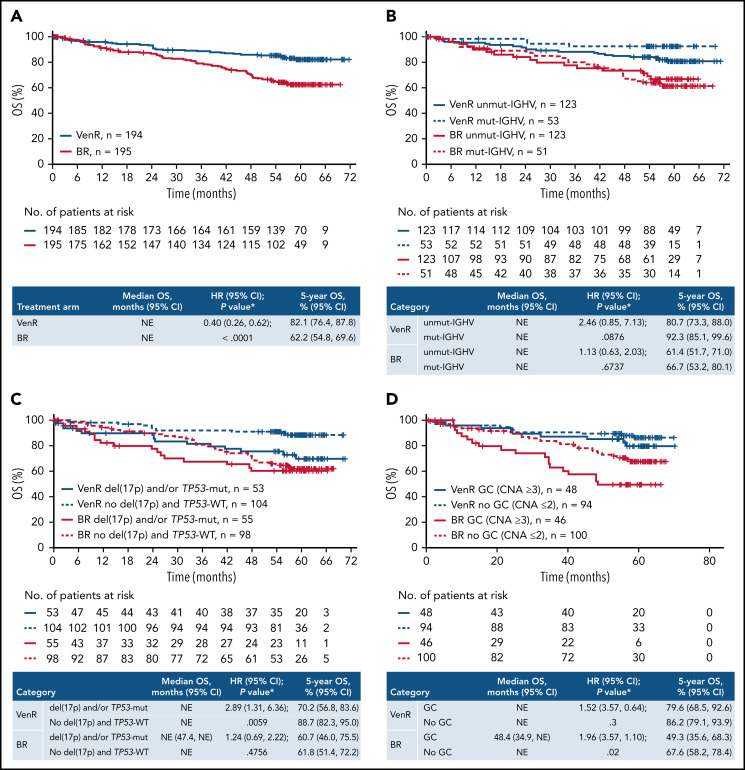
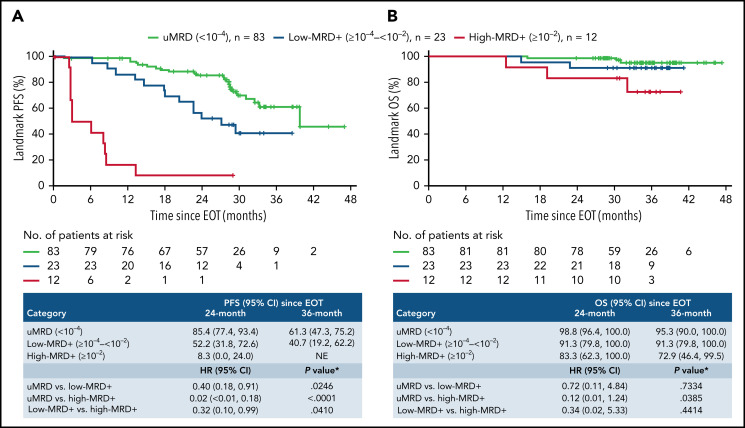
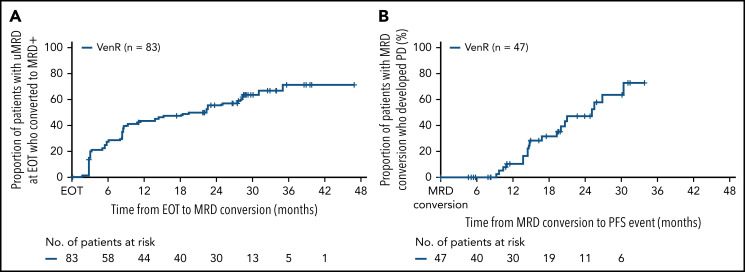
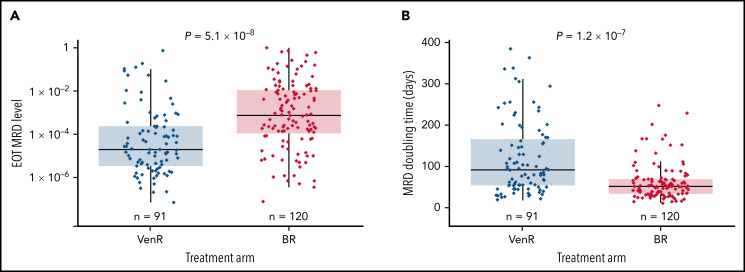
The MURANO trial (A Study to Evaluate the Benefit of Venetoclax Plus Rituximab Compared With Bendamustine Plus Rituximab in Participants With Relapsed or Refractory Chronic Lymphocytic Leukemia [CLL]; ClinicalTrials.gov identifier #NCT02005471) reported superior progression-free survival (PFS) and overall survival (OS) with venetoclax-rituximab (VenR) vs bendamustine-rituximab (BR) in relapsed/refractory (R/R) CLL. Patients were randomized to 2 years of VenR (n = 194; rituximab for the first 6 months) or 6 months of BR (n = 195). Although undetectable minimal residual disease (uMRD) was achieved more often with VenR, the long-term implications of uMRD with this fixed-duration, chemotherapy-free regimen have not been explored. We report MRD kinetics and updated outcomes with 5 years' follow-up. Survival benefits with VenR vs BR were sustained (median PFS [95% confidence interval]: 53.6 [48.4, 57.0] vs 17.0 [15.5, 21.7] months, respectively, P < .0001; 5-year OS [95% confidence interval]: 82.1% [76.4, 87.8] vs 62.2% [54.8, 69.6], P < .0001). VenR was superior to BR, regardless of cytogenetic category. VenR-treated patients with uMRD at end of treatment (EOT; n = 83) had superior OS vs those with high-MRD+ (n = 12): 3-year post-EOT survival rates were 95.3% vs 72.9% (P = .039). In those with uMRD at EOT, median time to MRD conversion was 19.4 months. Of 47 patients with documented MRD conversion, 19 developed progressive disease (PD); median time from conversion to PD was 25.2 months. A population-based logistic growth model indicated slower MRD median doubling time post-EOT with VenR (93 days) vs BR (53 days; P = 1.2 × 10-7). No new safety signals were identified. Sustained survival, uMRD benefits, and durable responses support 2-year fixed-duration VenR treatment in R/R CLL.
© 2022 by The American Society of Hematology.
Figures
Comment in
-
uMRD: "the" endpoint or "an" endpoint for CLL?Blood. 2022 Aug 25;140(8):797-798. doi: 10.1182/blood.2022016927. Blood. 2022. PMID: 36006672 No abstract available.
-
Measurable residual disease in Japanese patients with relapsed or refractory chronic lymphocytic leukemia treated with venetoclax.Int J Hematol. 2023 Oct;118(4):526-528. doi: 10.1007/s12185-023-03646-3. Epub 2023 Aug 15. Int J Hematol. 2023. PMID: 37581752 Free PMC article. No abstract available.
References
-
- European Medicines Agency . Appendix 4 to the guideline on the evaluation of anticancer medicinal products in man—condition specific guidance. Vol. Rev. 2. Ref number: EMA/CHMP/703715/2012; 2016. https://www.ema.europa.eu/en/documents/scientific-guideline/evaluation-a.... Accessed 25 May 2022.
-
- Böttcher S, Ritgen M, Fischer K, et al. . Minimal residual disease quantification is an independent predictor of progression-free and overall survival in chronic lymphocytic leukemia: a multivariate analysis from the randomized GCLLSG CLL8 trial. J Clin Oncol. 2012;30(9):980-988. - PubMed
-
- Hallek M, Cheson BD, Catovsky D, et al. . iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood. 2018;131(25):2745-2760. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
