

CD19/22 CAR T cells in children and young adults with B-ALL: phase 1 results and development of a novel bicistronic CAR
- PMID: 35605184
- PMCID: PMC9353146
- DOI: 10.1182/blood.2022015795
CD19/22 CAR T cells in children and young adults with B-ALL: phase 1 results and development of a novel bicistronic CAR
Abstract
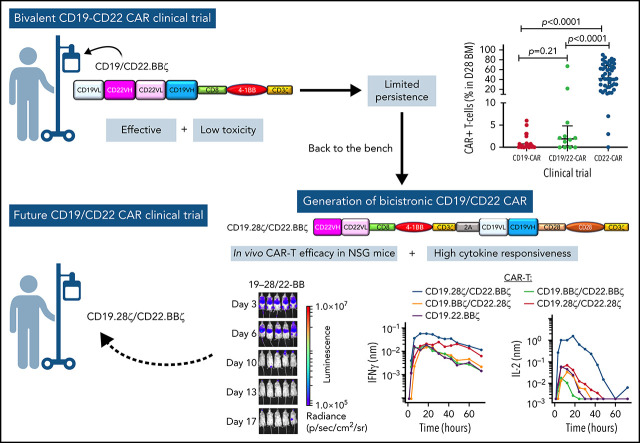
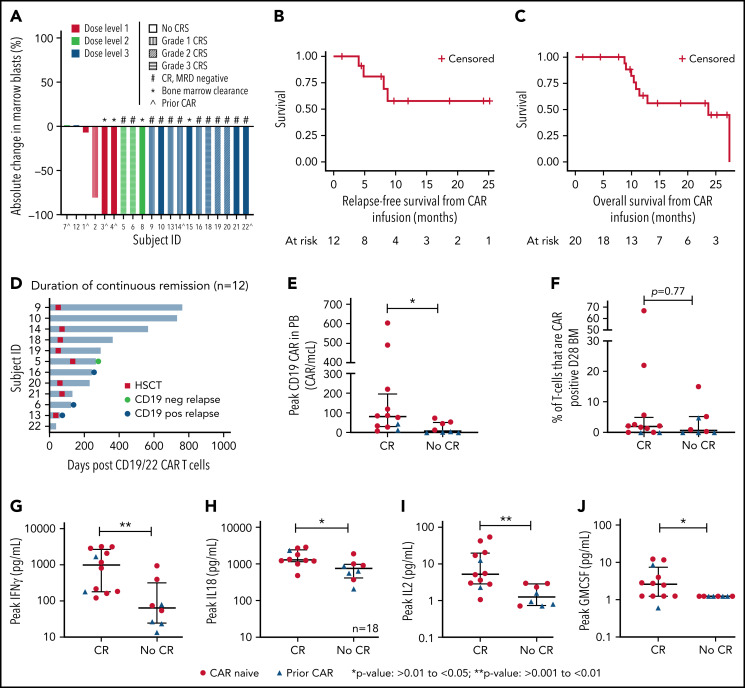
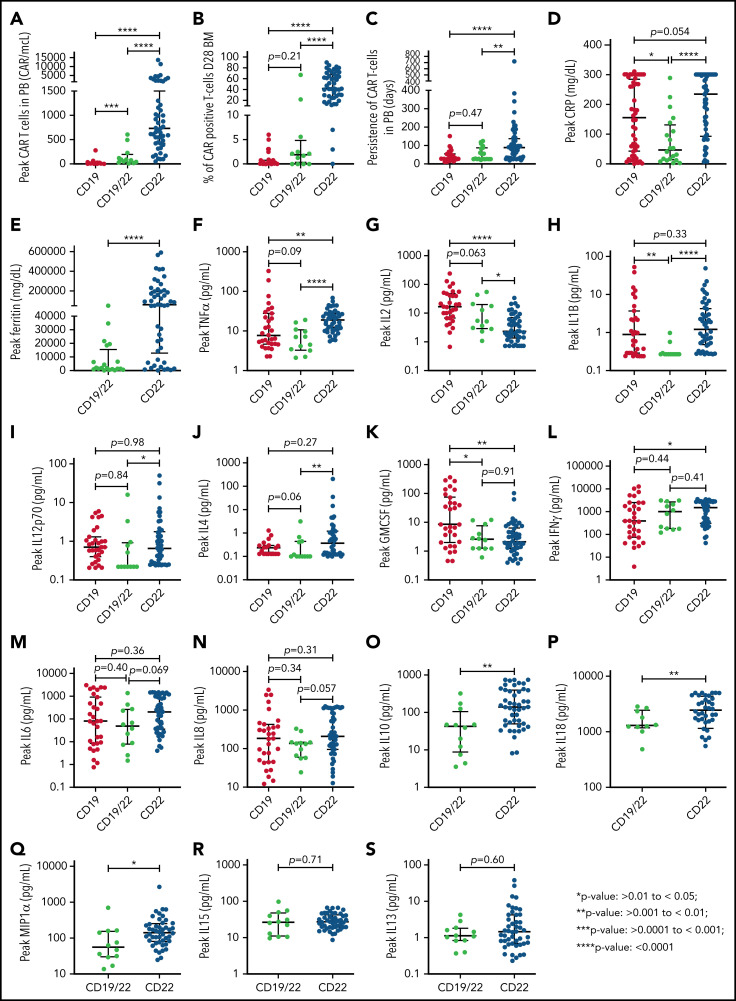
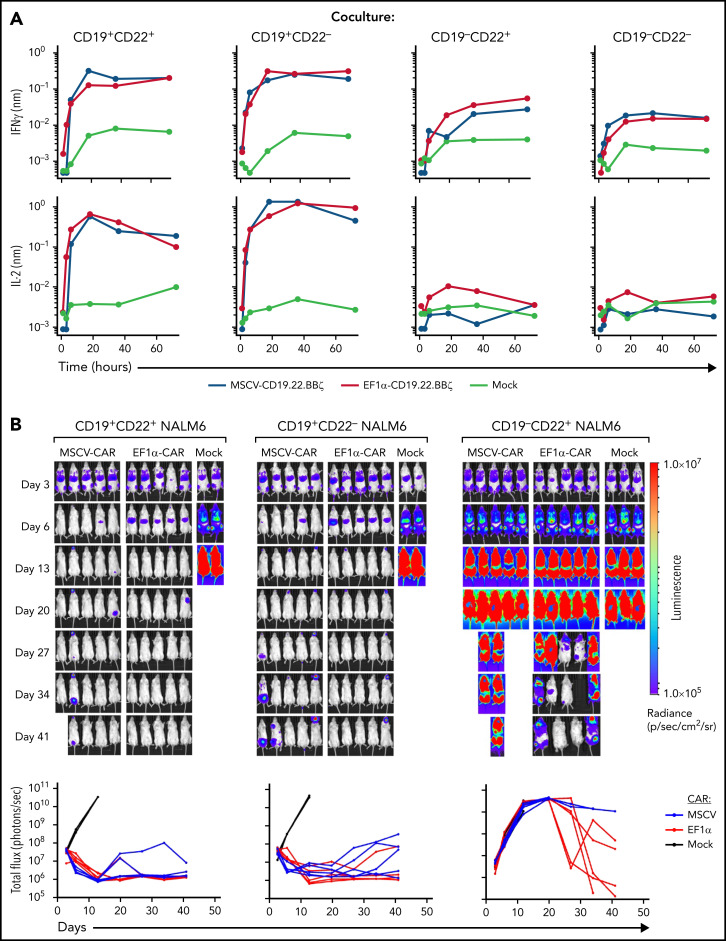
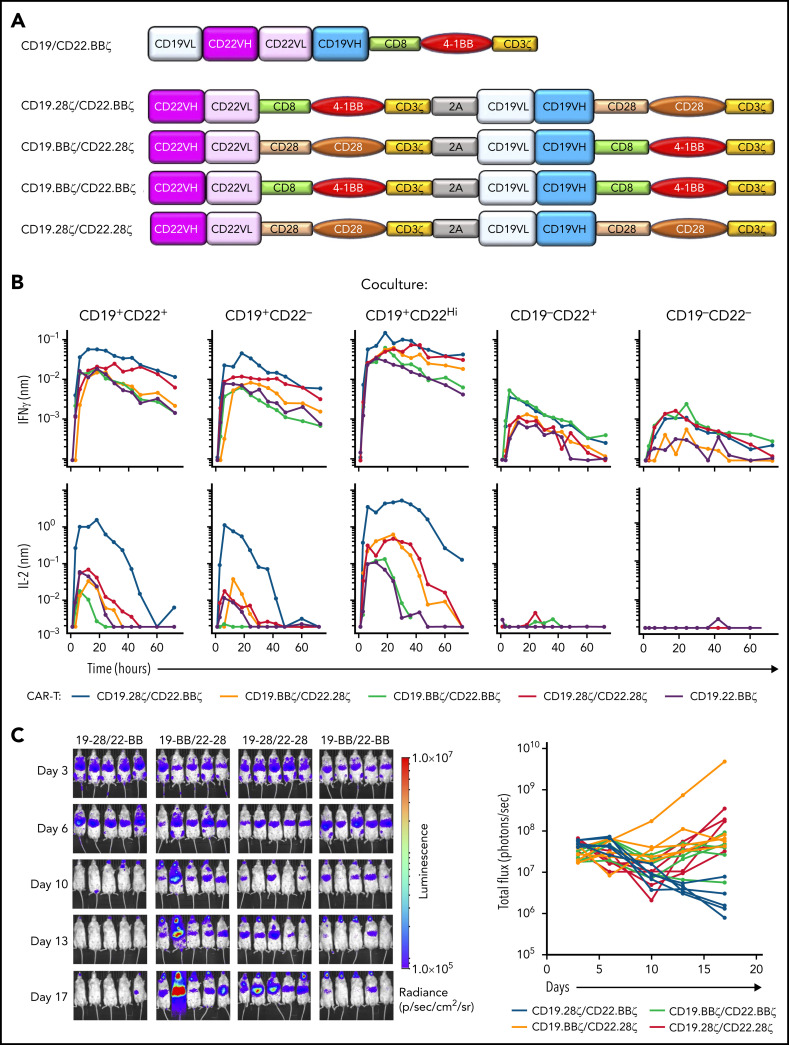
Remission durability following single-antigen targeted chimeric antigen receptor (CAR) T-cells is limited by antigen modulation, which may be overcome with combinatorial targeting. Building upon our experiences targeting CD19 and CD22 in B-cell acute lymphoblastic leukemia (B-ALL), we report on our phase 1 dose-escalation study of a novel murine stem cell virus (MSCV)-CD19/CD22-4-1BB bivalent CAR T-cell (CD19.22.BBζ) for children and young adults (CAYA) with B-cell malignancies. Primary objectives included toxicity and dose finding. Secondary objectives included response rates and relapse-free survival (RFS). Biologic correlatives included laboratory investigations, CAR T-cell expansion and cytokine profiling. Twenty patients, ages 5.4 to 34.6 years, with B-ALL received CD19.22.BBζ. The complete response (CR) rate was 60% (12 of 20) in the full cohort and 71.4% (10 of 14) in CAR-naïve patients. Ten (50%) developed cytokine release syndrome (CRS), with 3 (15%) having ≥ grade 3 CRS and only 1 experiencing neurotoxicity (grade 3). The 6- and 12-month RFS in those achieving CR was 80.8% (95% confidence interval [CI]: 42.4%-94.9%) and 57.7% (95% CI: 22.1%-81.9%), respectively. Limited CAR T-cell expansion and persistence of MSCV-CD19.22.BBζ compared with EF1α-CD22.BBζ prompted laboratory investigations comparing EF1α vs MSCV promoters, which did not reveal major differences. Limited CD22 targeting with CD19.22.BBζ, as evaluated by ex vivo cytokine secretion and leukemia eradication in humanized mice, led to development of a novel bicistronic CD19.28ζ/CD22.BBζ construct with enhanced cytokine production against CD22. With demonstrated safety and efficacy of CD19.22.BBζ in a heavily pretreated CAYA B-ALL cohort, further optimization of combinatorial antigen targeting serves to overcome identified limitations (www.clinicaltrials.gov #NCT03448393).
© 2022 by The American Society of Hematology.
Figures
Comment in
-
Reverse translational studies inform dual-targeted CAR T-cell design.Blood. 2022 Aug 4;140(5):409-410. doi: 10.1182/blood.2022016928. Blood. 2022. PMID: 35925644 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
