

Treatment of Osteochondral Lesions of the Talus in the Skeletally Immature Population: A Systematic Review
- PMID: 35605211
- PMCID: PMC9351694
- DOI: 10.1097/BPO.0000000000002175
Treatment of Osteochondral Lesions of the Talus in the Skeletally Immature Population: A Systematic Review
Abstract
Introduction: Skeletally immature osteochondral lesions of the talus (OLTs) are underreported and little is known about the clinical efficacy of different treatment options. The primary aim of the present study was to investigate the clinical efficacy of different conservative and surgical treatment options. The secondary aim was to assess return to sports (RTS) and radiologic outcomes for the different treatment options.
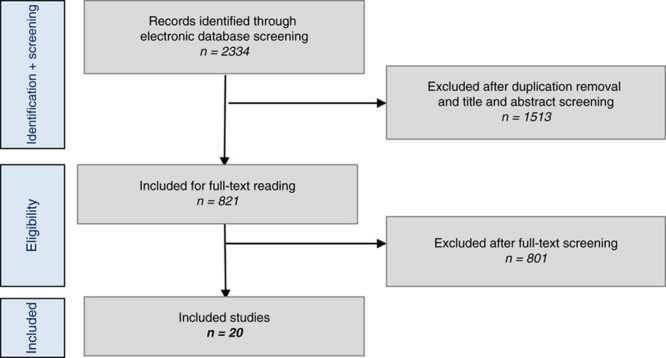
Methods: An electronic literature search was carried out in the databases PubMed, EMBASE, Cochrane, CDSR, CENTRAL, and DARE from January 1996 to September 2021 to identify suitable studies for this review. The authors separately screened the articles for eligibility and conducted the quality assessment using the Methodological Index for Non-Randomized Studies (MINORS). Clinical success rates were calculated per separate study and pooled per treatment strategy. Radiologic outcomes and sports outcomes for the different treatment strategies were assessed.
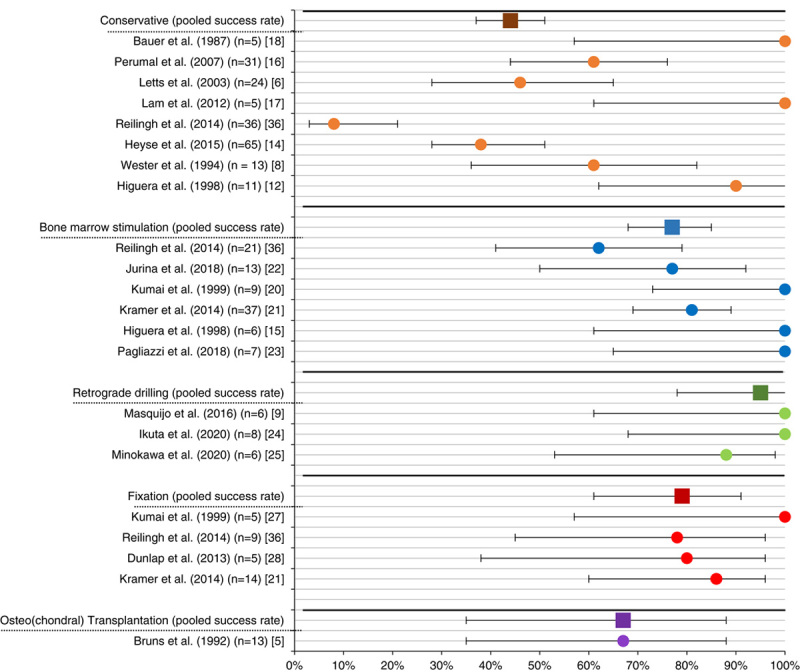
Results: Twenty studies with a total of 381 lesions were included. The mean MINORS score of the included study was 7.6 (range: 5 to 9). The pooled success rate was 44% [95% confidence interval (CI): 37%-51%] in the conservative group (n=192), 77% (95% CI: 68%-85%) in the bone marrow stimulation (BMS) group (n=97), 95% (95% CI: 78%-99%) in the retrograde drilling (RD) group (n=22), 79% (95% CI: 61%-91%) in the fixation group (n=33) and 67% (95% CI: 35%-88%) in the osteo(chondral) autograft group (n=9). RTS rates were reported in 2 treatment groups: BMS showed an RTS rate of 86% (95% CI: 42%-100%) without specified levels and an RTS rate to preinjury level of 43% (95% CI: 10%-82%). RD showed an RTS rate of 100% (95% CI: 63%-100%) without specified levels, an RTS rate to preinjury level was not given. RTS times were not given for any treatment option. The radiologic success according to magnetic resonance imaging were 29% (95% CI: 16%-47%) (n=31) in the conservative group, 81% (95% CI: 65%-92%) (n=37) in the BMS group, 41% (95% CI: 18%-67%) (n=19) in the RD group, 87% (95% CI: 65%-97%) (n=19) in the fixation group, and were not reported in the osteo(chondral) transplantation group. Radiologic success rates based on computed tomography scans were 62% (95% CI: 32%-86%) (n=13) in the conservative group, 30% (95% CI: 7%-65%) (n=10) in the BMS group, 57% (95% CI: 25%-84%) (n=7) in the RD group, and were not reported for the fixation and the osteo(chondral) transplantation groups.
Conclusions: This study showed that for skeletally immature patients presenting with symptomatic OLTs, conservative treatment is clinically successful in 4 out of 10 children, whereas the different surgical treatment options were found to be successful in 7 to 10 out of 10 children. Specifically, fixation was clinically successful in 8 out of 10 patients and showed radiologically successful outcomes in 9 out of 10 patients, and would therefore be the primary preferred surgical treatment modality. The treatment provided should be tailor-made, considering lesion characteristics and patient and parent preferences.
Level of evidence: Level IV-systematic review and meta-analysis.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Evidence-based Treatment of Failed Primary Osteochondral Lesions of the Talus: A Systematic Review on Clinical Outcomes of Bone Marrow Stimulation.Cartilage. 2021 Dec;13(1_suppl):1411S-1421S. doi: 10.1177/1947603521996023. Epub 2021 Feb 22. Cartilage. 2021. PMID: 33618537 Free PMC article.
-
Satisfactory long-term clinical outcomes after bone marrow stimulation of osteochondral lesions of the talus.Knee Surg Sports Traumatol Arthrosc. 2021 Nov;29(11):3525-3533. doi: 10.1007/s00167-021-06630-8. Epub 2021 Jun 29. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 34185110 Free PMC article. Review.
-
Return to Sports After Surgical Treatment of Osteochondral Defects of the Talus: A Systematic Review of 2347 Cases.Orthop J Sports Med. 2019 Oct 22;7(10):2325967119876238. doi: 10.1177/2325967119876238. eCollection 2019 Oct. Orthop J Sports Med. 2019. PMID: 31673563 Free PMC article. Review.
-
Adequate return to sports and sports activities after treatment of Lisfranc injury: a meta-analysis.J ISAKOS. 2021 Jul;6(4):212-219. doi: 10.1136/jisakos-2020-000477. Epub 2020 Dec 10. J ISAKOS. 2021. PMID: 34272297
-
Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis.Cartilage. 2024 Feb 7:19476035241227332. doi: 10.1177/19476035241227332. Online ahead of print. Cartilage. 2024. PMID: 38323533 Free PMC article.
Cited by
-
Osteochondritis dissecans in children: location-dependent differences (part II: ankle and elbow).Pediatr Radiol. 2025 Jun;55(7):1386-1402. doi: 10.1007/s00247-025-06259-6. Epub 2025 May 16. Pediatr Radiol. 2025. PMID: 40377713 Review.
-
Juvenile Osteochondral Lesions of the Talus: Current Concepts Review and an Update on the Literature.Children (Basel). 2023 May 15;10(5):884. doi: 10.3390/children10050884. Children (Basel). 2023. PMID: 37238431 Free PMC article. Review.
-
Casting and rehabilitation versus skillful neglect for osteochondral lesions of the talus in the pediatric population: the care study, a multicenter, prospective comparative study.BMC Musculoskelet Disord. 2025 May 15;26(1):481. doi: 10.1186/s12891-025-08646-4. BMC Musculoskelet Disord. 2025. PMID: 40375271 Free PMC article.
-
All Arthroscopic Osteochondral Autograft Transplantation for Medial Talar Dome Lesions Talus With Burring of the Anterior Lip of the Distal Tibia.Arthrosc Tech. 2024 Aug 29;13(11):103109. doi: 10.1016/j.eats.2024.103109. eCollection 2024 Nov. Arthrosc Tech. 2024. PMID: 39711893 Free PMC article.
-
Physician preferences in diagnostics and treatment of juvenile osteochondritis dissecans are diverse across the knee, ankle and elbow: an ESSKA survey.Knee Surg Sports Traumatol Arthrosc. 2023 Nov;31(11):5228-5237. doi: 10.1007/s00167-023-07563-0. Epub 2023 Oct 3. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 37787862 Free PMC article.
References
-
- Rikken QGH, Kerkhoffs GMMJ. Osteochondral Lesions of the Talus: An Individualized Treatment Paradigm from the Amsterdam Perspective. Foot Ankle Clin. 2021;26:121–136. - PubMed
-
- Bruns J, Rosenbach B. Osteochondrosis dissecans of the talus. Comparison of results of surgical treatment in adolescents and adults. Arch Orthop Trauma Surg. 1992;112:23–27. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
