

A Longitudinal Study of COVID-19 Sequelae and Immunity: Baseline Findings
- PMID: 35605238
- PMCID: PMC9128805
- DOI: 10.7326/M21-4905
A Longitudinal Study of COVID-19 Sequelae and Immunity: Baseline Findings
Abstract
Background: A substantial proportion of persons who develop COVID-19 report persistent symptoms after acute illness. Various pathophysiologic mechanisms have been implicated in the pathogenesis of postacute sequelae of SARS-CoV-2 infection (PASC).
Objective: To characterize medical sequelae and persistent symptoms after recovery from COVID-19 in a cohort of disease survivors and controls.
Design: Cohort study. (ClinicalTrials.gov: NCT04411147).
Setting: National Institutes of Health Clinical Center, Bethesda, Maryland.
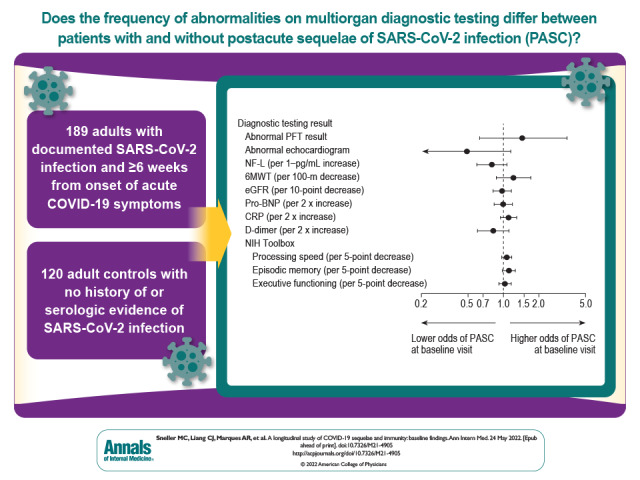
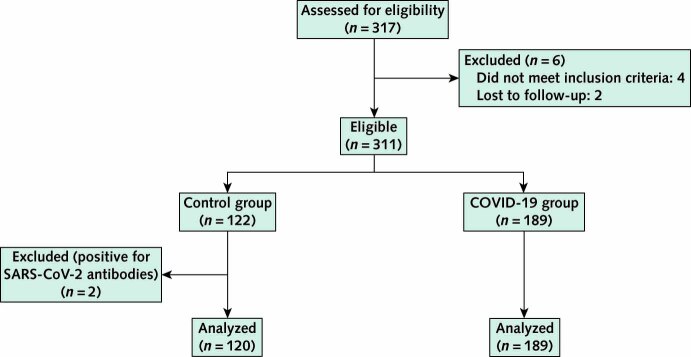
Participants: Self-referred adults with laboratory-documented SARS-CoV-2 infection who were at least 6 weeks from symptom onset were enrolled regardless of presence of PASC. A control group comprised persons with no history of COVID-19 or serologic evidence of SARS-CoV-2 infection, recruited regardless of their current health status. Both groups were enrolled over the same period and from the same geographic area.
Measurements: All participants had the same evaluations regardless of presence of symptoms, including physical examination, laboratory tests and questionnaires, cognitive function testing, and cardiopulmonary evaluation. A subset also underwent exploratory immunologic and virologic evaluations.
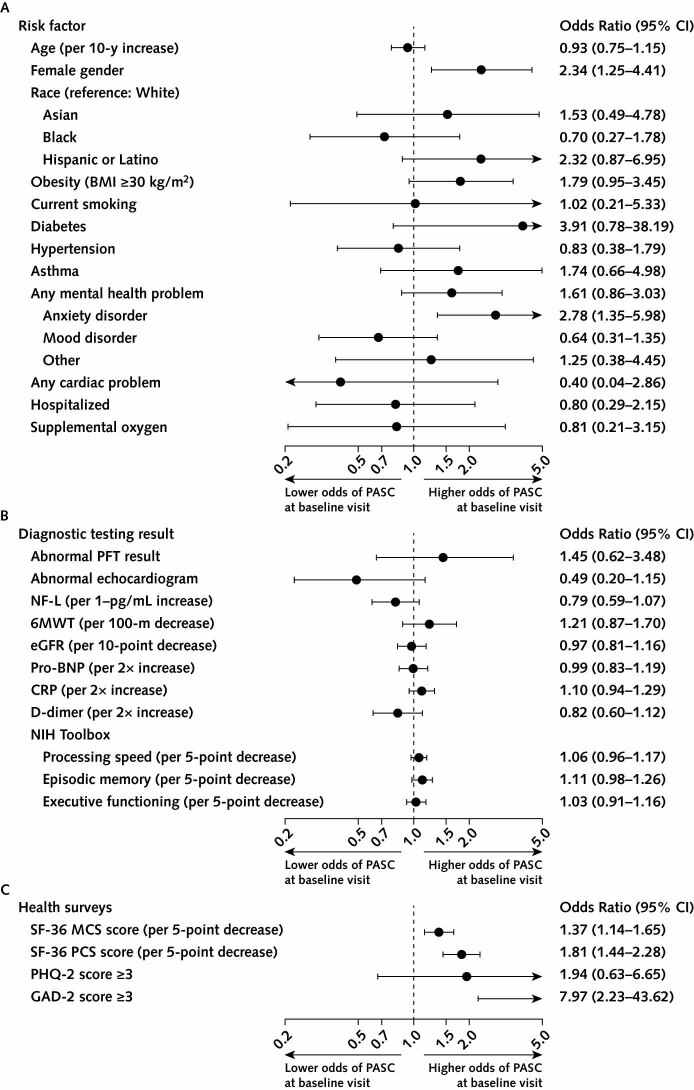
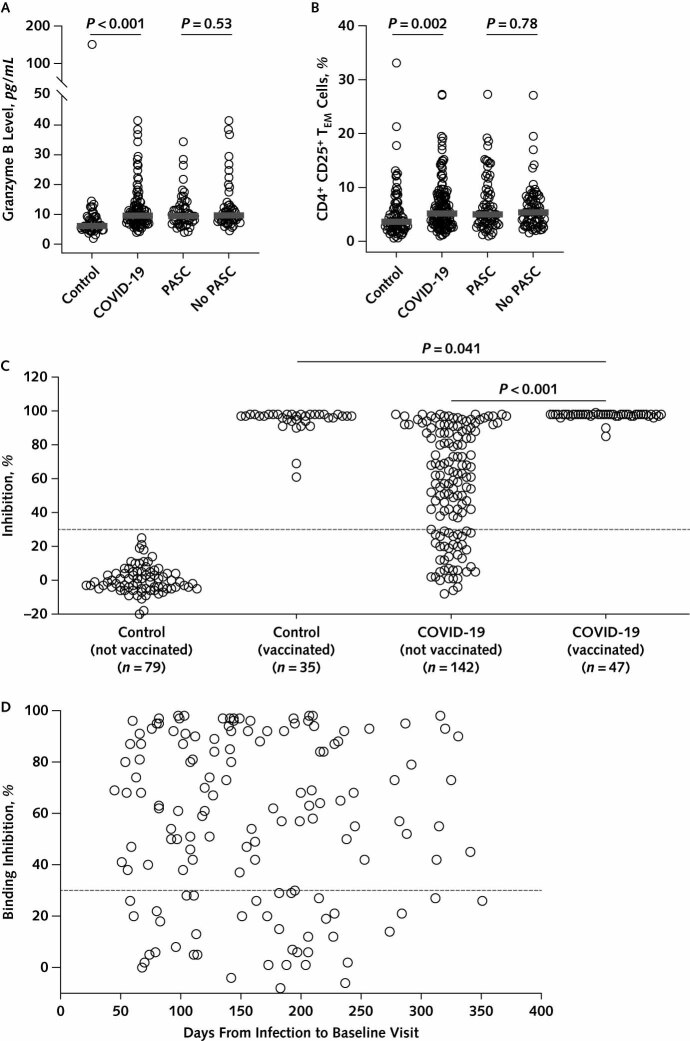
Results: 189 persons with laboratory-documented COVID-19 (12% of whom were hospitalized during acute illness) and 120 antibody-negative control participants were enrolled. At enrollment, symptoms consistent with PASC were reported by 55% of the COVID-19 cohort and 13% of control participants. Increased risk for PASC was noted in women and those with a history of anxiety disorder. Participants with findings meeting the definition of PASC reported lower quality of life on standardized testing. Abnormal findings on physical examination and diagnostic testing were uncommon. Neutralizing antibody levels to spike protein were negative in 27% of the unvaccinated COVID-19 cohort and none of the vaccinated COVID-19 cohort. Exploratory studies found no evidence of persistent viral infection, autoimmunity, or abnormal immune activation in participants with PASC.
Limitations: Most participants with COVID-19 had mild to moderate acute illness that did not require hospitalization. The prevalence of reported PASC was likely overestimated in this cohort because persons with PASC may have been more motivated to enroll. The study did not capture PASC that resolved before enrollment.
Conclusion: A high burden of persistent symptoms was observed in persons after COVID-19. Extensive diagnostic evaluation revealed no specific cause of reported symptoms in most cases. Antibody levels were highly variable after COVID-19.
Primary funding source: Division of Intramural Research, National Institute of Allergy and Infectious Diseases.
Conflict of interest statement
Figures
Comment in
-
Understanding and Improving Recovery From COVID-19.Ann Intern Med. 2022 Jul;175(7):1041-1042. doi: 10.7326/M22-1492. Epub 2022 May 24. Ann Intern Med. 2022. PMID: 35605242 No abstract available.
-
A Longitudinal Study of COVID-19 Sequelae and Immunity.Ann Intern Med. 2022 Dec;175(12):W153. doi: 10.7326/L22-0330. Epub 2022 Nov 1. Ann Intern Med. 2022. PMID: 36315942 No abstract available.
-
A Longitudinal Study of COVID-19 Sequelae and Immunity.Ann Intern Med. 2022 Dec;175(12):W153. doi: 10.7326/L22-0331. Epub 2022 Nov 1. Ann Intern Med. 2022. PMID: 36315947 No abstract available.
References
-
- World Health Organization. COVID-19 Weekly Epidemiological Update. Edition 87. 12 April 2022.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous