

Impact of MRD status in patients with AML undergoing allogeneic stem cell transplantation in the first vs the second remission
- PMID: 35605254
- PMCID: PMC9636320
- DOI: 10.1182/bloodadvances.2022007168
Impact of MRD status in patients with AML undergoing allogeneic stem cell transplantation in the first vs the second remission
Abstract
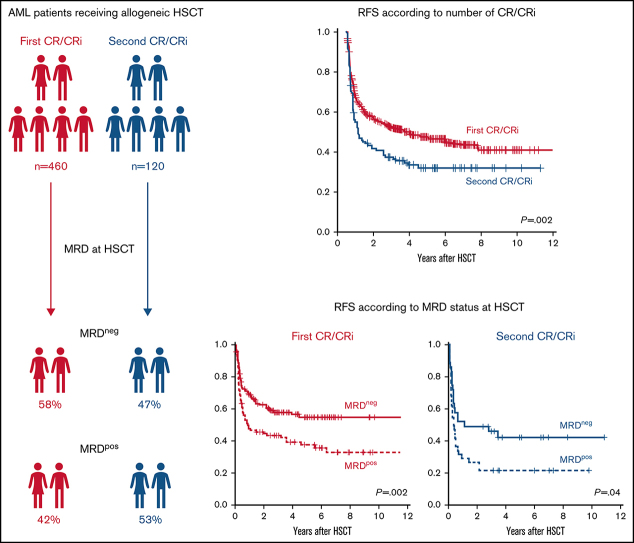
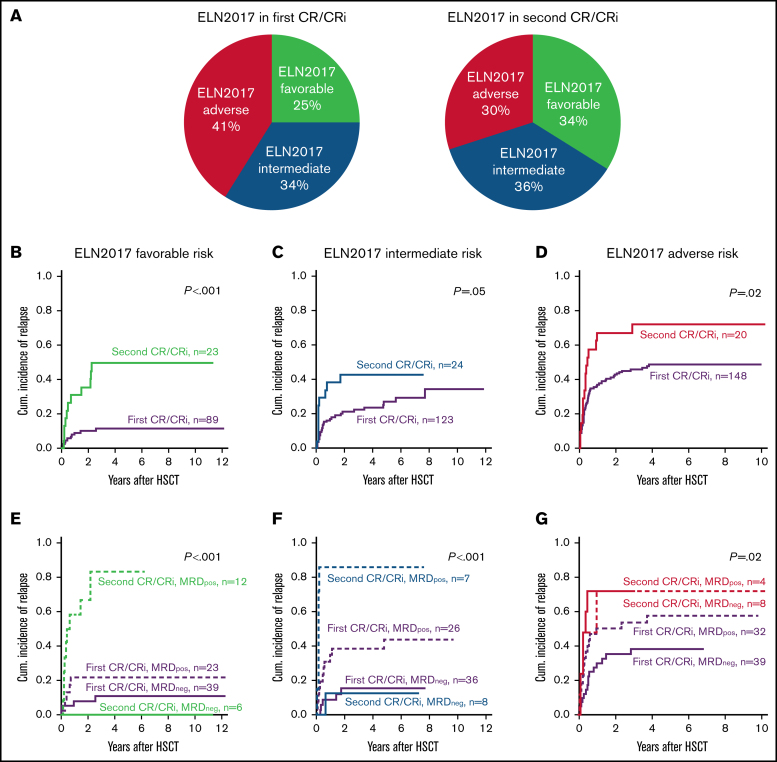
Allogeneic hematopoietic stem cell transplantation (HSCT) offers the best chance for relapse-free survival to most patients with acute myeloid leukemia (AML). It may be performed during complete remission or delayed until after the first relapse because of relevant treatment-related morbidity and mortality. The measurable residual disease (MRD) status at HSCT adds refined prognostic information to the assigned European LeukemiaNet (ELN) 2017 genetic risk at diagnosis. We analyzed 580 patients with AML who underwent allogeneic HSCT during either the first (79%) or second (21%) remission. Although, because of common treatment strategies, some adverse risk characteristics, such as monosomal or complex karyotypes, were less frequent in patients who underwent transplant in the second remission, those patients had worse outcomes compared with patients who had transplant in the first remission. The MRD status at HSCT was an independent prognostic factor, irrespective of the number of remissions at HSCT. Notably, patients who were MRD+ who underwent HSCT in the first remission and those who were MRD- and underwent transplant in the second remission had similar outcomes. In the clinically highly relevant group of individuals who had ELN2017 intermediate risk, the MRD status provided the highest prognostic value with very dismal outcomes for patients who were MRD+ and underwent second-remission transplants. The adverse outcomes of patients who are MRD+ and of those who undergo transplant in the second remission should be considered when planning consolidation treatment, to avert an allogeneic HSCT in MRD+ second remission when possible.
© 2022 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Figures


References
-
- Cornelissen JJ, Gratwohl A, Schlenk RF, et al. The European LeukemiaNet AML Working Party consensus statement on allogeneic HSCT for patients with AML in remission: an integrated-risk adapted approach. Nat Rev Clin Oncol. 2012;9(10):579–590. - PubMed
-
- Cornelissen JJ, van Putten WLJ, Verdonck LF, et al. Results of a HOVON/SAKK donor versus no-donor analysis of myeloablative HLA-identical sibling stem cell transplantation in first remission acute myeloid leukemia in young and middle-aged adults: benefits for whom? Blood. 2007;109(9):3658–3666. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
