

COVID-19 vaccine booster dose needed to achieve Omicron-specific neutralisation in nursing home residents
- PMID: 35605428
- PMCID: PMC9122310
- DOI: 10.1016/j.ebiom.2022.104066
COVID-19 vaccine booster dose needed to achieve Omicron-specific neutralisation in nursing home residents
Abstract
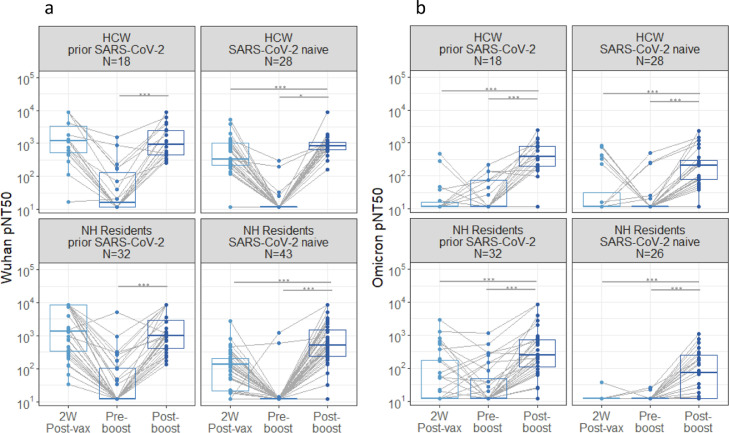
Background: Nursing home (NH) residents have borne a disproportionate share of SARS-CoV-2 morbidity and mortality. Vaccines have limited hospitalisation and death from earlier variants in this vulnerable population. With the rise of Omicron and future variants, it is vital to sustain and broaden vaccine-induced protection. We examined the effect of boosting with BNT162b2 mRNA vaccine on humoral immunity and Omicron-specific neutralising activity among NH residents and healthcare workers (HCWs).
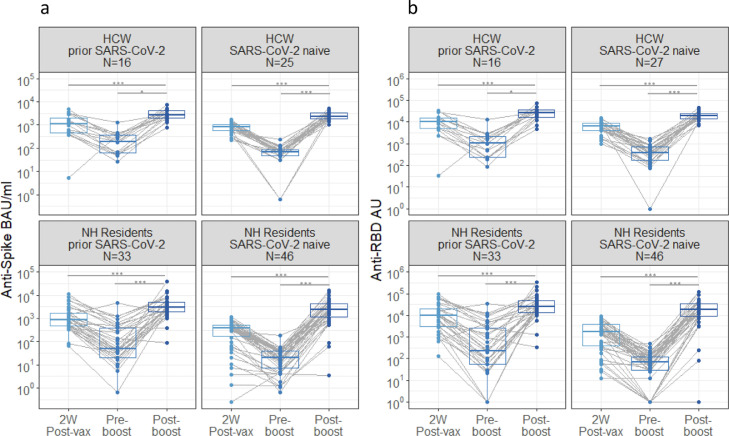
Methods: We longitudinally enrolled 85 NH residents (median age 77) and 48 HCWs (median age 51), and sampled them after the initial vaccination series; and just before and 2 weeks after booster vaccination. Anti-spike, anti-receptor binding domain (RBD) and neutralisation titres to the original Wuhan strain and neutralisation to the Omicron strain were obtained.
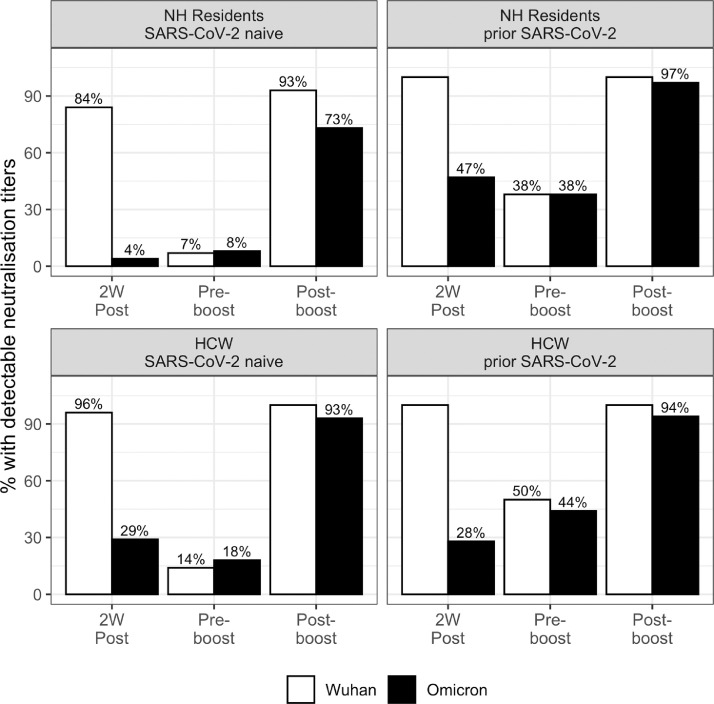
Findings: Booster vaccination significantly increased vaccine-specific anti-spike, anti-RBD, and neutralisation levels above the pre-booster levels in NH residents and HCWs, both in those with and without prior SARS-CoV-2 infection. Omicron-specific neutralisation activity was low after the initial 2 dose series with only 28% of NH residents' and 28% HCWs' titres above the assay's lower limit of detection. Omicron neutralising activity following the booster lifted 86% of NH residents and 93% of HCWs to the detectable range.
Interpretation: With boosting, the vast majority of HCWs and NH residents developed detectable Omicron-specific neutralising activity. These data provide immunologic evidence that strongly supports booster vaccination to broaden neutralising activity and counter waning immunity in the hope it will better protect this vulnerable, high-risk population against the Omicron variant.
Funding: NIH AI129709-03S1, U01 CA260539-01, CDC 200-2016-91773, and VA BX005507-01.
Keywords: Booster; COVID-19; Geriatrics; Long-term care; Omicron; Vaccination.
Published by Elsevier B.V.
Conflict of interest statement
S. G. and D. H. C. are recipients of investigator-initiated grants to their universities from Pfizer to study pneumococcal vaccines and Sanofi Pasteur and Seqirus to study influenza vaccines. S. G. also does consulting for Janssen, Merck, Moderna, Novavax, Pfizer, Sanofi, Seqirus, and Vaxart; and, has served on the speaker's bureaus for Seqirus and Sanofi; and paid to chair data safety monitoring boards from Longevoron and SciClone. D. H. C. has done consulting work for Seqirus.
Figures
Update of
-
Significantly elevated antibody levels and neutralization titers in nursing home residents after SARS-CoV-2 BNT162b2 mRNA booster vaccination.medRxiv [Preprint]. 2021 Dec 7:2021.12.07.21267179. doi: 10.1101/2021.12.07.21267179. medRxiv. 2021. Update in: EBioMedicine. 2022 Jun;80:104066. doi: 10.1016/j.ebiom.2022.104066. PMID: 34909792 Free PMC article. Updated. Preprint.
References
-
- Nursing Home Covid-19 Data Dashboard. 2022. https://www.cdc.gov/nhsn/covid19/ltc-report-overview.html#anchor_1594393304.
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
