

IgG4-positive plasma cells in nonspecific sialadenitis and sialolithiasis
- PMID: 35606412
- PMCID: PMC9514989
- DOI: 10.1038/s41379-022-01089-5
IgG4-positive plasma cells in nonspecific sialadenitis and sialolithiasis
Abstract
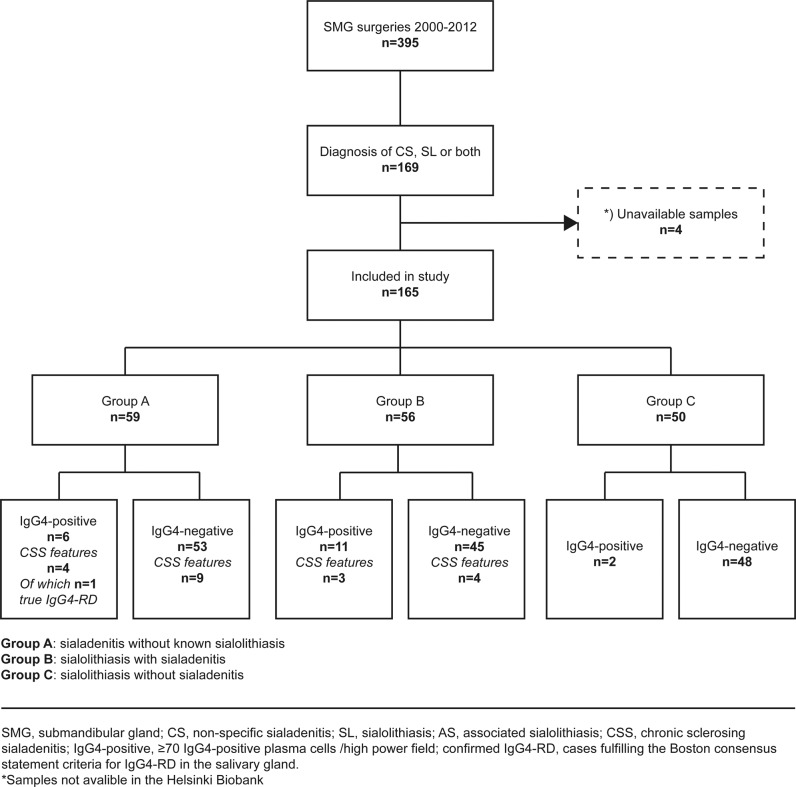
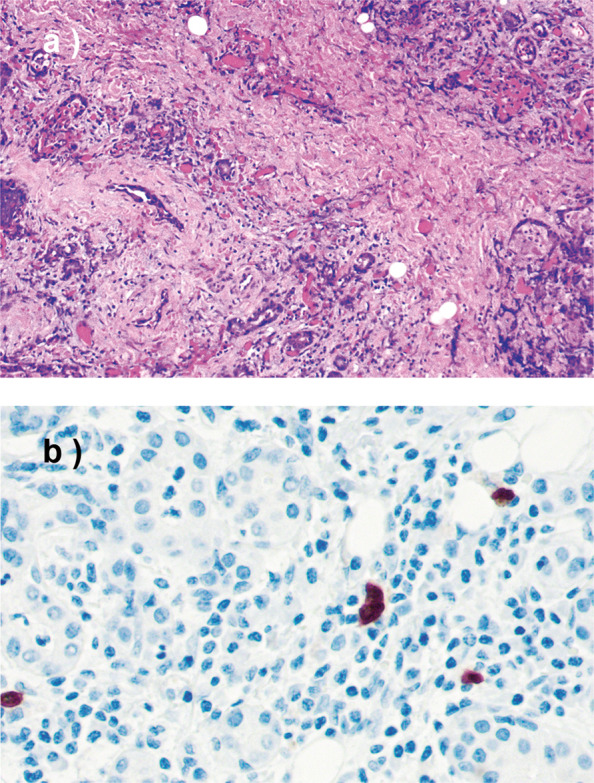
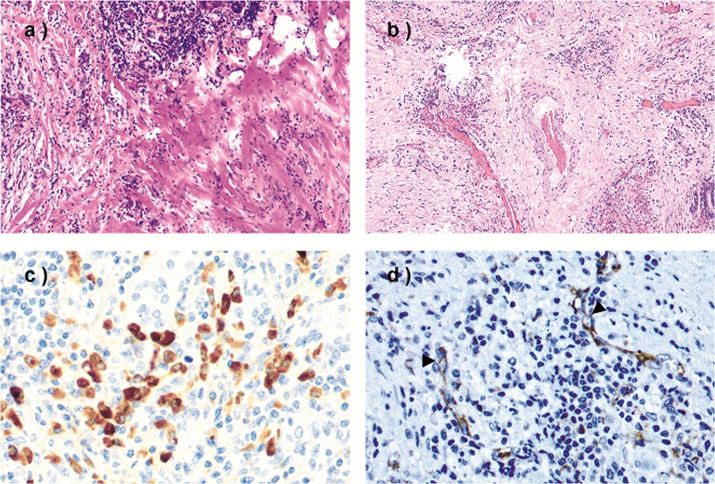
Chronic sclerosing sialadenitis is commonly regarded as a manifestation of IgG4-related disease. We previously found that a high IgG4 expression or IgG4-related disease could accompany nonspecific sialadenitis, whereas chronic sclerosing sialadenitis was not directly associated with IgG4-related disease. Our previous findings lead us to hypothesize that these inflammatory conditions of the submandibular gland signify a continuous progression of disease rather than different disease entities. We, therefore, aimed to determine the presence of IgG4-positivity and genuine IgG4-related disease in a cohort of 165 submandibular gland specimens from patients who underwent surgery due to chronic nonspecific sialadenitis or sialolithiasis. To do so, we re-evaluated histopathological features and divided samples into three groups: (A) nonspecific sialadenitis without known sialolithiasis, (B) sialadenitis with sialolithiasis, and (C) sialolithiasis without sialadenitis. We performed immunohistochemical staining for IgG4, IgG, and CD31, and assessed the Boston consensus statement criteria for IgG4-related disease in IgG4-positive samples. We also reviewed patient records and supplemented follow-up data with a questionnaire among patients with IgG4-positive samples. IgG4-positive plasma cells (range 1-344) were found in 131 samples. Among these, 19 samples were classified as IgG4-positive (≥70 IgG4-positive plasma cells/high-power field). Two IgG4-positive samples were histologically highly suggestive of IgG4-related disease, but only one had a clinically confirmed diagnosis of IgG4-related disease. Our results indicate that patients with sialadenitis and sialolithiasis often present with IgG4-positive lymphoplasmacytic infiltrates, but exceedingly rarely present with genuine IgG4-related disease. In sialolithiasis without sialadenitis, IgG4-positive plasma cells are often absent or appear in small numbers. These results support our hypothesis of a continuum of disease, and indicate that progressive inflammation of the submandibular gland leads to the development of more specific pathological features over time.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Toll-like receptors 2 and 4, and bacterial proteins in IgG4-related sialadenitis, other types of chronic sialadenitis and sialolithiasis.J Oral Microbiol. 2024 Jul 24;16(1):2382633. doi: 10.1080/20002297.2024.2382633. eCollection 2024. J Oral Microbiol. 2024. PMID: 39055281 Free PMC article.
-
Sclerosing sialadenitis of the submandibular gland is rarely an immunoglobulin G4-related disease in the Finnish population.Mod Pathol. 2020 Apr;33(4):551-559. doi: 10.1038/s41379-019-0395-5. Epub 2019 Nov 3. Mod Pathol. 2020. PMID: 31680120
-
Chronic sclerosing sialadenitis (Küttner tumor) is an IgG4-associated disease.Am J Surg Pathol. 2010 Feb;34(2):202-10. doi: 10.1097/PAS.0b013e3181c811ad. Am J Surg Pathol. 2010. PMID: 20061932
-
Immunoglobulin G4-related sclerosing sialadenitis: report of two cases and review of the literature.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Oct;108(4):544-50. doi: 10.1016/j.tripleo.2009.06.001. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009. PMID: 19778741 Review.
-
The 2023 revised diagnostic criteria for IgG4-related dacryoadenitis and sialadenitis.Mod Rheumatol. 2025 Apr 8;35(3):542-547. doi: 10.1093/mr/roae096. Mod Rheumatol. 2025. PMID: 39441008 Review.
Cited by
-
Viral DNA in submandibular gland tissue with an inflammatory disorder.J Oral Microbiol. 2024 Apr 26;16(1):2345941. doi: 10.1080/20002297.2024.2345941. eCollection 2024. J Oral Microbiol. 2024. PMID: 38711909 Free PMC article.
-
Toll-like receptors 2 and 4, and bacterial proteins in IgG4-related sialadenitis, other types of chronic sialadenitis and sialolithiasis.J Oral Microbiol. 2024 Jul 24;16(1):2382633. doi: 10.1080/20002297.2024.2382633. eCollection 2024. J Oral Microbiol. 2024. PMID: 39055281 Free PMC article.
-
Chronic sclerosing sialadenitis of the bilateral submandibular glands in childhood - a diagnostic dilemma.Rom J Morphol Embryol. 2024 Jan-Mar;65(1):113-118. doi: 10.47162/RJME.65.1.14. Rom J Morphol Embryol. 2024. PMID: 38527991 Free PMC article.
-
Chronic Sclerosing Sialadenitis of the Submandibular Gland and its Histopathological Spectrum in the IgG4-Related Disease: a Series of 17 Cases.Head Neck Pathol. 2024 May 13;18(1):42. doi: 10.1007/s12105-024-01651-4. Head Neck Pathol. 2024. PMID: 38735890 Free PMC article.
-
IgG4-related disease: an update on pathology and diagnostic criteria with a focus on salivary gland manifestations.Virchows Arch. 2024 Mar;484(3):381-399. doi: 10.1007/s00428-024-03757-0. Epub 2024 Feb 5. Virchows Arch. 2024. PMID: 38316669 Review.
References
-
- Geyer JT, Deshpande V. IgG4-associated sialadenitis. Curr Opin Rheumatol. 23, 95-101 (2011) - PubMed
-
- Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 366, 539-51 (2012) - PubMed
-
- Laco J, Ryska A, Celakovsky P, Dolezalova H, Mottl R, Tucek L. Chronic sclerosing sialadenitis as one of the immunoglobulin G4-related diseases: a clinicopathological study of six cases from Central Europe. Histopathology. 58, 1157-63 (2011) - PubMed
-
- Peuraharju E, Saarinen R, Aro K, Mäkinen LK, Tarkkanen J, Mäkitie A et al. Sclerosing sialadenitis of the submandibular gland is rarely an immunoglobulin G4-related disease in the Finnish population. Mod Pathol. 33, 551-559 (2020) - PubMed
