

Early postoperative endoscopic evaluation of rectal anastomoses: a prospective cross-sectional study
- PMID: 35606545
- PMCID: PMC9652211
- DOI: 10.1007/s00464-022-09323-6
Early postoperative endoscopic evaluation of rectal anastomoses: a prospective cross-sectional study
Abstract
Background: Reported incidence of anastomotic leakage (AL) of rectal anastomoses is up to 29% with an overall mortality up to 12%. Nevertheless, there is no uniform evidence-based diagnostic procedure for early detection of AL. The objective of this prospective clinical trial was to demonstrate the diagnostic value of early postoperative flexible endoscopy for rectal anastomosis evaluation.
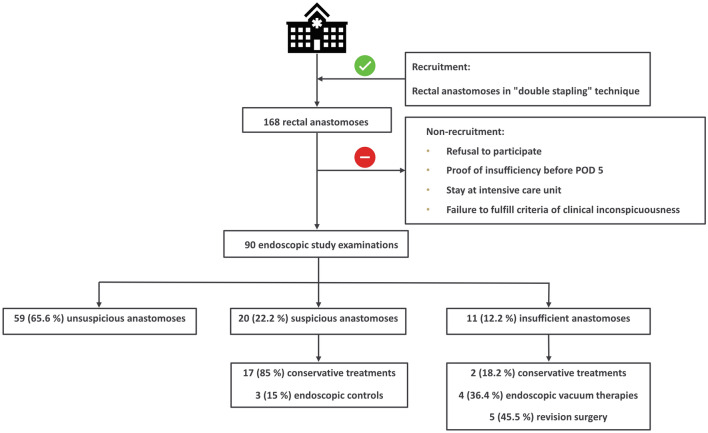
Methods: Flexible endoscopy between 5 and 8th postoperative day was performed consecutively in 90 asymptomatic patients. Sample size calculation was made using the two-stage Simon design. Diagnostic value was measured by management change after endoscopic evaluation. Anastomoses were categorized according to a new classification. Study is registered in German Clinical Trials Register (DRKS00019217).
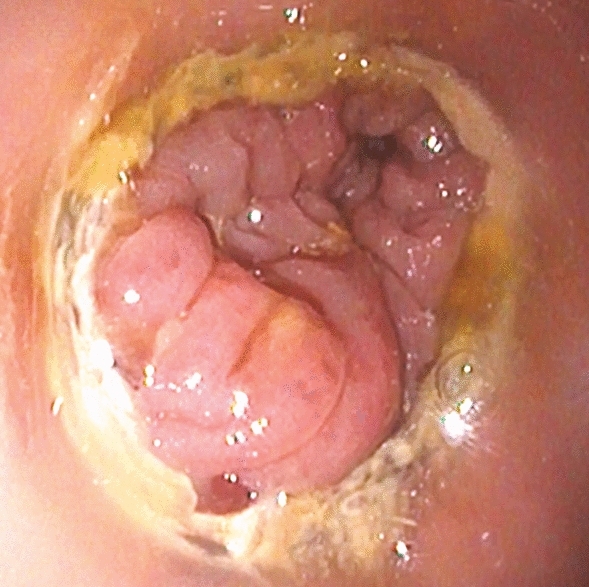
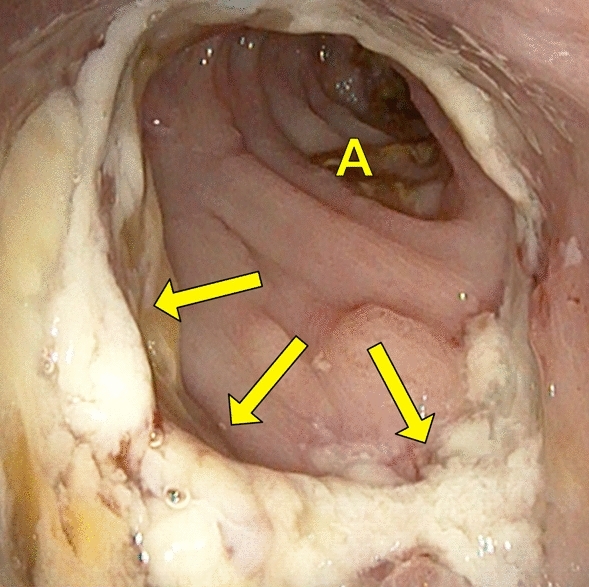
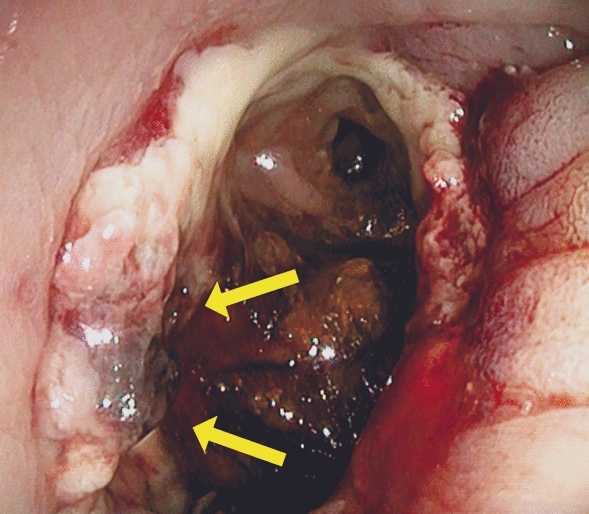
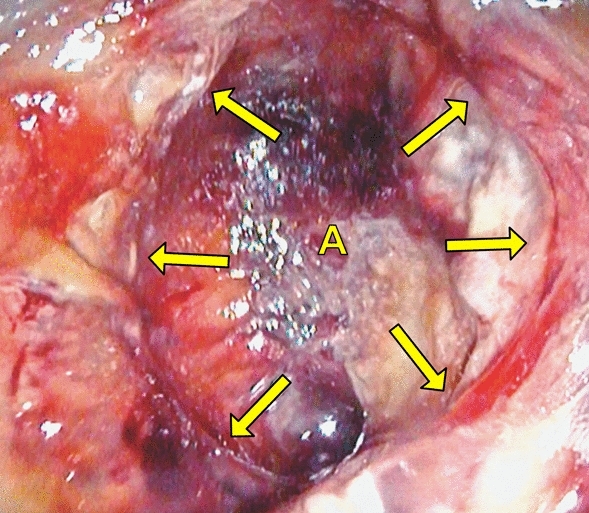
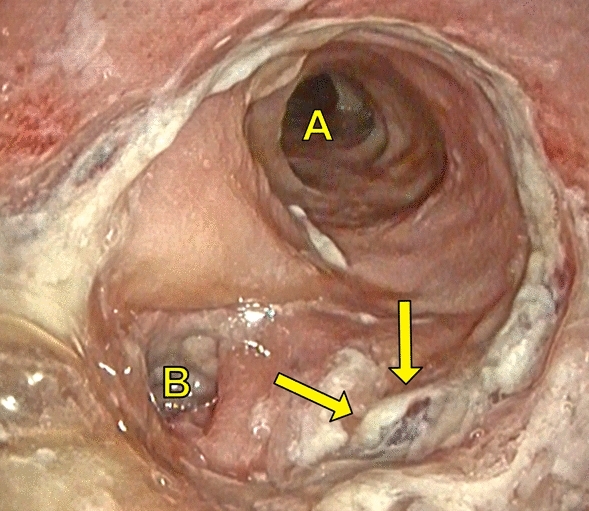
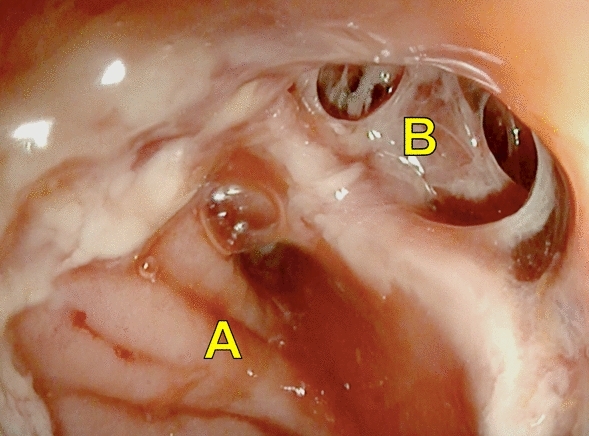
Results: Of the 90 anastomoses, 59 (65.6%) were unsuspicious. 20 (22.2%) were suspicious with partial fibrin plaques (n = 15), intramural hematoma and/or local blood coagulum (n = 4) and ischemic area in one. 17 of these anastomoses were treated conservatively under monitoring. In three a further endoscopic re-evaluation was performed and as consequence one patient underwent endoscopic vacuum therapy. 11 (12.2%) AL were detected. Here, two could be treated conservatively under monitoring, four with endoscopic vacuum therapy and five needed revision surgery. No intervention-related adverse events occurred. A change in postoperative management was made in 31 (34.4%) patients what caused a significant improvement of diagnosis of AL (p < 0.001).
Conclusions: Early postoperative endoscopic evaluation of rectal anastomoses is a safe procedure thus allows early detection of AL. Early treatment for suspicious anastomoses or AL could be adapted to avoid severe morbidity and mortality.
Keywords: Anastomotic leakage; Colorectal anastomosis; Colorectal surgery; Flexible endoscopy; Postoperative management.
© 2022. The Author(s).
Conflict of interest statement
Steffen Axt, Kristin Haller, Peter Wilhelm, Claudius Falch, Peter Martus, Jonas Johannink, Jens Rolinger, Christian Beltzer, Lena Axt, Alfred Königsrainer, and Andreas Kirschniak have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Rahbari NN, Weitz J, Hohenberger W, Heald RJ, Moran B, Ulrich A, Holm T, Wong WD, Tiret E, Moriya Y, Laurberg S, den Dulk M, van de Velde C, Buchler MW. Definition and grading of anastomotic leakage following anterior resection of the rectum: a proposal by the International Study Group of Rectal Cancer. Surgery. 2010;147:339–351. doi: 10.1016/j.surg.2009.10.012. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
