

International virtual confidential reviews of infection-related maternal deaths and near-miss in 11 low- and middle-income countries - case report series and suggested actions
- PMID: 35606709
- PMCID: PMC9128080
- DOI: 10.1186/s12884-022-04731-x
International virtual confidential reviews of infection-related maternal deaths and near-miss in 11 low- and middle-income countries - case report series and suggested actions
Abstract
Background: Obstetric infections are the third most common cause of maternal mortality, with the largest burden in low and middle-income countries (LMICs). We analyzed causes of infection-related maternal deaths and near-miss identified contributing factors and generated suggested actions for quality of care improvement.
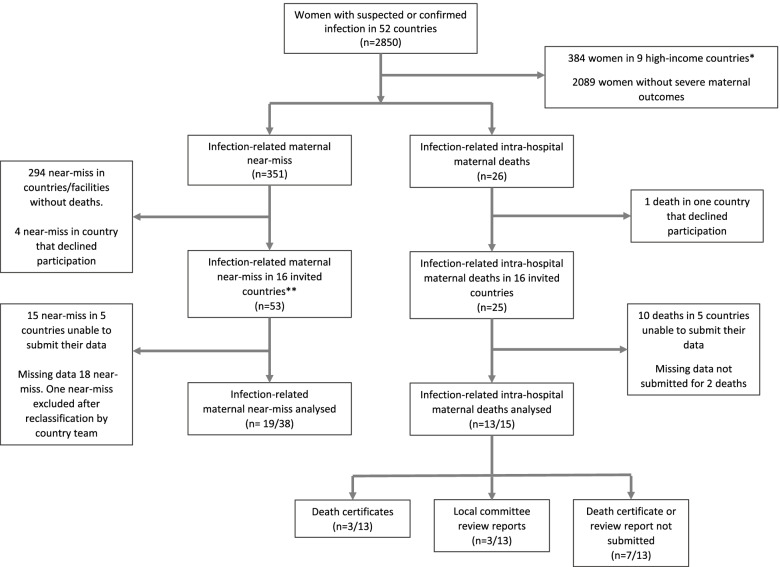
Method: An international, virtual confidential enquiry was conducted for maternal deaths and near-miss cases that occurred in 15 health facilities in 11 LMICs reporting at least one death within the GLOSS study. Facility medical records and local review committee documents containing information on maternal characteristics, timing and chain of events, case management, outcomes, and facility characteristics were summarized into a case report for each woman and reviewed by an international external review committee. Modifiable factors were identified and suggested actions were organized using the three delays framework.
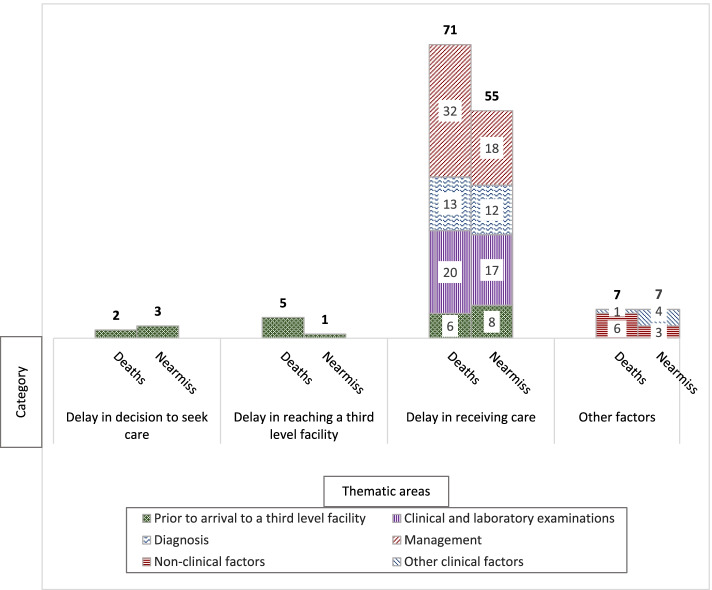
Results: Thirteen infection-related maternal deaths and 19 near-miss cases were reviewed in 20 virtual meetings by an international external review committee. Of 151 modifiable factors identified during the review, delays in receiving care contributed to 71/85 modifiable factors in maternal deaths and 55/66 modifiable factors in near-miss cases. Delays in reaching a GLOSS facility contributed to 5/85 and 1/66 modifiable factors for maternal deaths and near-miss cases, respectively. Two modifiable factors in maternal deaths were related to delays in the decision to seek care compared to three modifiable factors in near-miss cases. Suboptimal use of antibiotics, missing microbiological culture and other laboratory results, incorrect working diagnosis, and infrequent monitoring during admission were the main contributors to care delays among both maternal deaths and near-miss cases. Local facility audits were conducted for 2/13 maternal deaths and 0/19 near-miss cases. Based on the review findings, the external review committee recommended actions to improve the prevention and management of maternal infections.
Conclusion: Prompt recognition and treatment of the infection remain critical addressable gaps in the provision of high-quality care to prevent and manage infection-related severe maternal outcomes in LMICs. Poor uptake of maternal death and near-miss reviews suggests missed learning opportunities by facility teams. Virtual platforms offer a feasible solution to improve routine adoption of confidential maternal death and near-miss reviews locally.
Keywords: Audit; Infections; Maternal death; Near-miss; Perinatal; Virtual.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Souza JP, Gülmezoglu AM, Vogel J, Carroli G, Lumbiganon P, Qureshi Z, et al. Moving beyond essential interventions for reduction of maternal mortality (the WHO multicountry survey on maternal and newborn health): a cross-sectional study. Lancet Lond Engl. 2013;381:1747–1755. doi: 10.1016/S0140-6736(13)60686-8. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
