

Joint-Specific Memory and Sustained Risk for New Joint Accumulation in Autoimmune Arthritis
- PMID: 35606924
- PMCID: PMC9617751
- DOI: 10.1002/art.42240
Joint-Specific Memory and Sustained Risk for New Joint Accumulation in Autoimmune Arthritis
Abstract
Objective: Inflammatory arthritides exhibit hallmark patterns of affected and spared joints, but in each individual, arthritis affects only a subset of all possible sites. The purpose of this study was to identify patient-specific patterns of joint flare to distinguish local from systemic drivers of disease chronicity.
Methods: Patients with juvenile idiopathic arthritis followed without interruption from disease onset into adulthood were identified across 2 large academic centers. Joints inflamed at each visit were established by medical record review. Flare was defined as physician-confirmed joint inflammation following documented inactive disease.
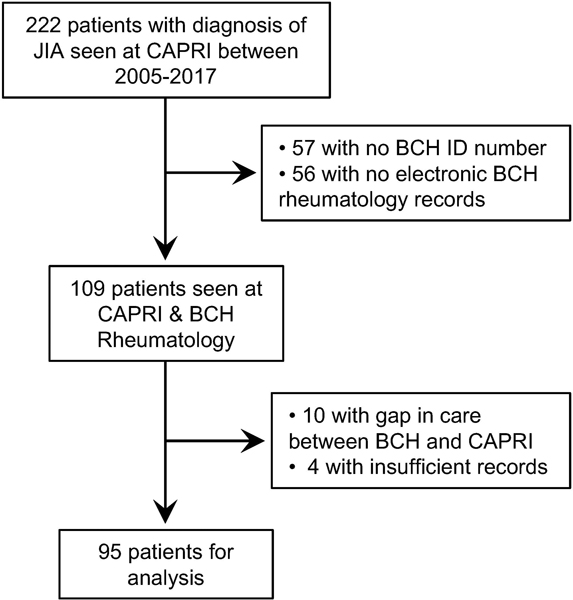
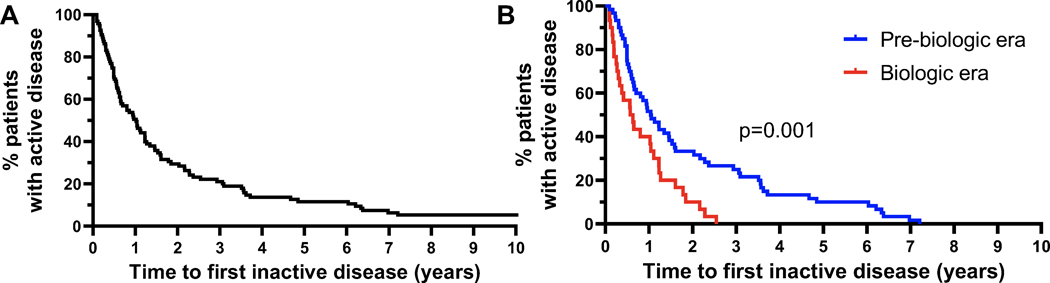
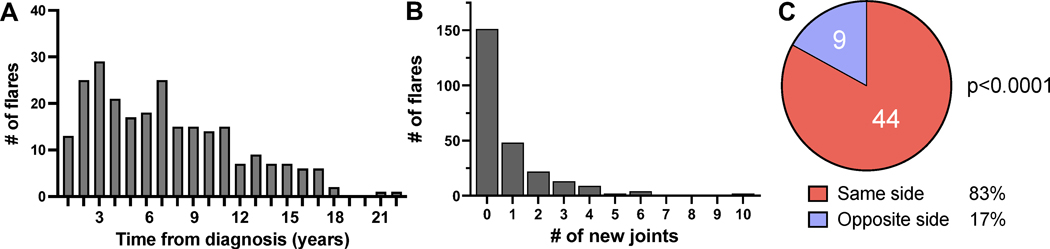
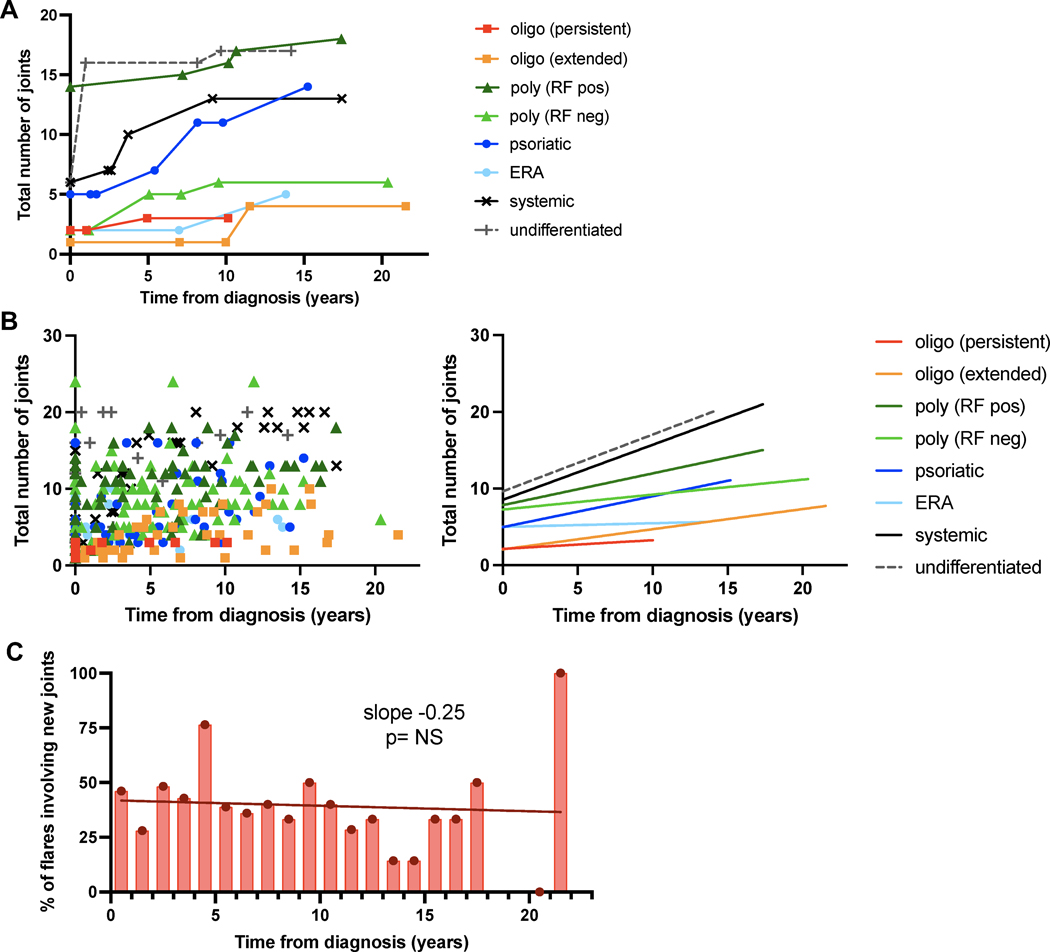
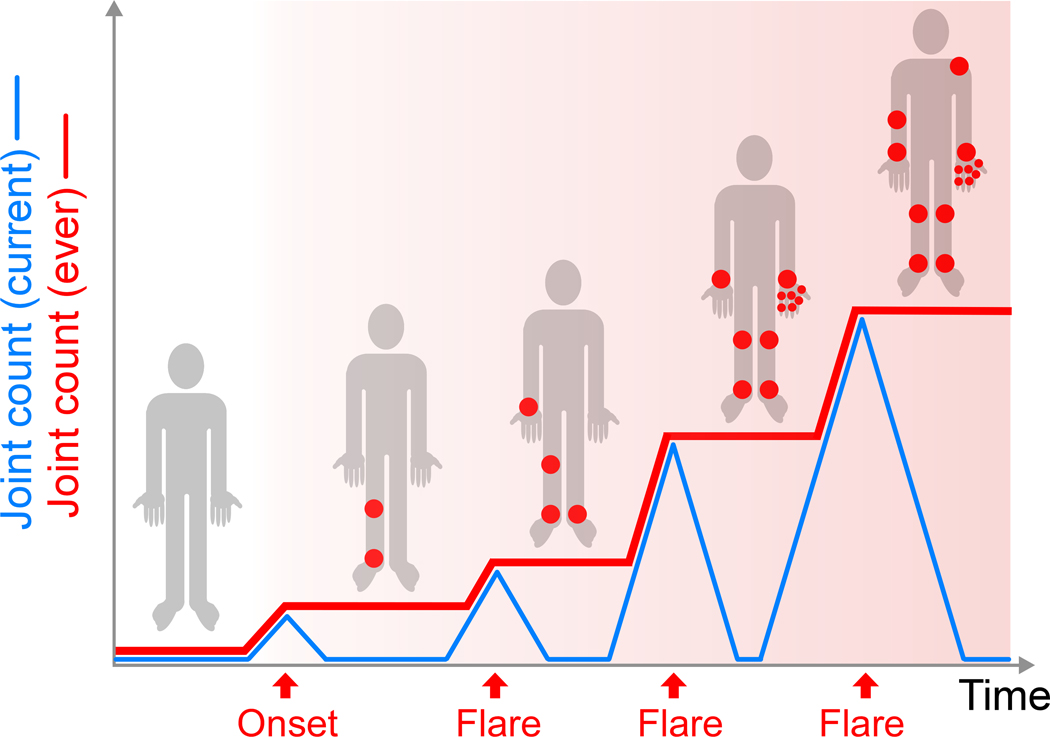
Results: Among 222 adults with JIA, 95 had complete serial joint examinations dating from disease onset in childhood. Mean follow-up was 12.5 years (interquartile range 7.9-16.7 years). Ninety (95%) of 95 patients achieved inactive disease, after which 81% (73 patients) experienced at least 1 flare. Among 940 joints affected in 253 flares, 74% had been involved previously. In flares affecting easily observed large joint pairs where only 1 side had been involved before (n = 53), the original joint was affected in 83% and the contralateral joint in 17% (P < 0.0001 versus random laterality). However, disease extended to at least 1 new joint in ~40% of flares, a risk that remained stable even decades after disease onset, and was greatest in flares that occurred while patients were not receiving medication (54% versus 36% of flares occurring with therapy; odds ratio 2.09, P = 0.015).
Conclusion: Arthritis flares preferentially affect previously inflamed joints but carry an ongoing risk of disease extension. These findings confirm joint-specific memory and suggest that prevention of new joint accumulation should be an important target for arthritis therapy.
© 2022 American College of Rheumatology.
Conflict of interest statement
Figures
References
-
- Roberts WN, Daltroy LH, and Anderson RJ. Stability of normal joint findings in persistent classic rheumatoid arthritis. Arthritis Rheum. 1988;31(2):267–71. - PubMed
-
- Heckert SL, Bergstra SA, Matthijssen XME, Goekoop-Ruiterman YPM, Fodili F, Ten Wolde S, et al. Joint inflammation tends to recur in the same joints during the rheumatoid arthritis disease course. Ann Rheum Dis. 2021. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
