

Rhythm-Monitoring Strategy and Arrhythmia Recurrence in Atrial Fibrillation Ablation Trials: A Systematic Review
- PMID: 35607484
- PMCID: PMC9123375
- DOI: 10.1016/j.cjco.2022.02.001
Rhythm-Monitoring Strategy and Arrhythmia Recurrence in Atrial Fibrillation Ablation Trials: A Systematic Review
Abstract
Background: : The rhythm-monitoring strategy after catheter ablation (CA) for atrial fibrillation (AF) impacts the detection of atrial arrhythmia recurrence and is not well characterized. We performed a systematic review and meta-regression analysis to determine whether the duration and mode of rhythm monitoring after CA affects detection of atrial arrhythmia recurrence.
Methods: Databases were systematically searched for randomized controlled trials of adult patients undergoing first CA for AF from 2007 to 2021. Duration and strategy of rhythm monitoring were extracted. Meta-regression was used to identify any association between duration of monitoring and detection of atrial arrhythmia recurrence. The primary measure of outcome was single-procedure recurrence of atrial arrhythmia.
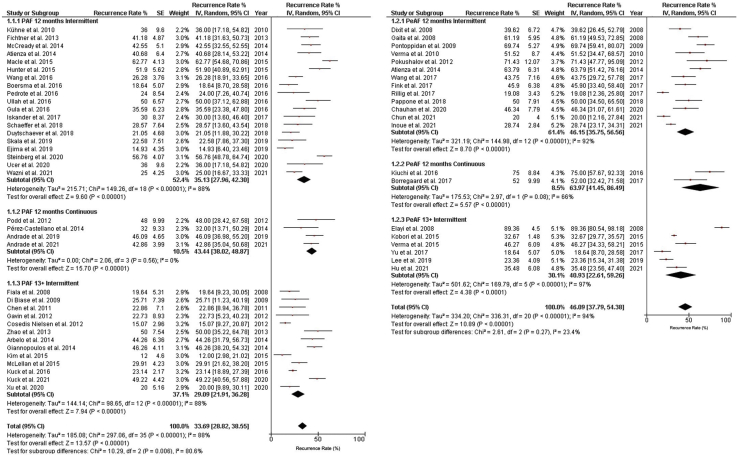
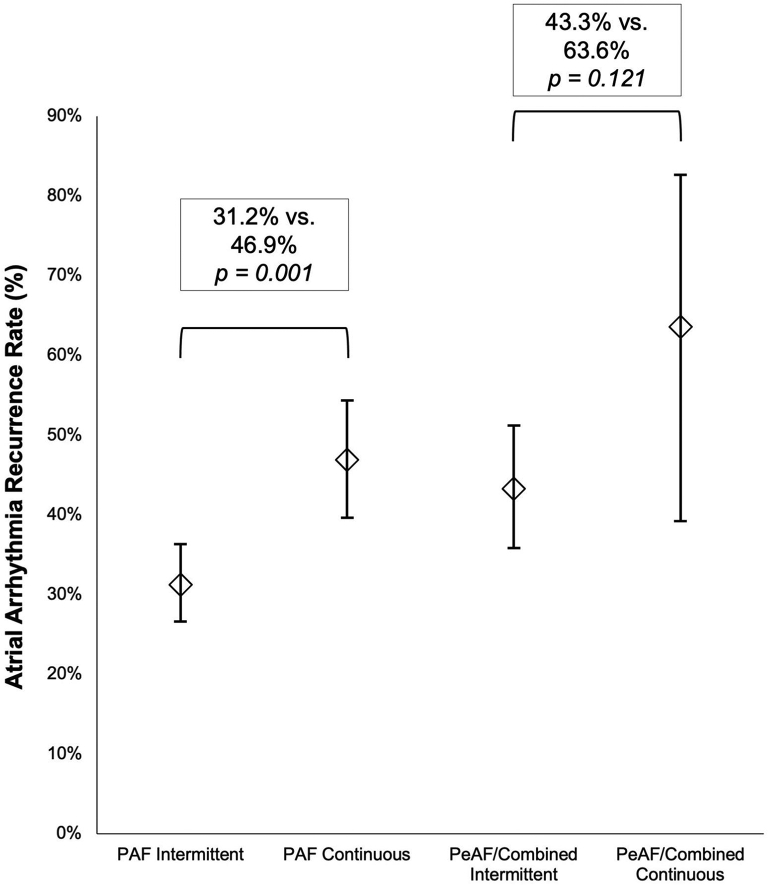
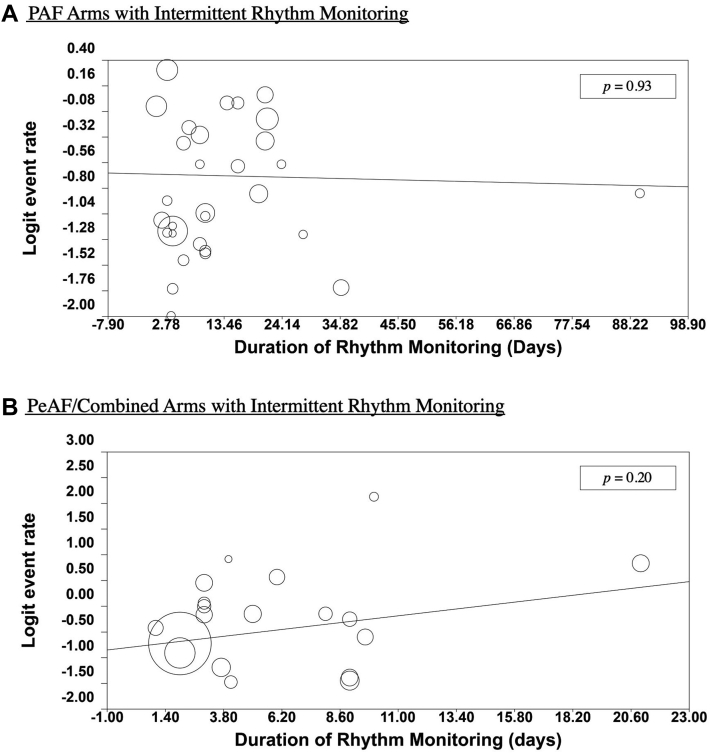
Results: The search strategy yielded 57 trial arms from 56 randomized controlled trials comprising 5322 patients: 36 arms of patients with paroxysmal AF (PAF), and 21 arms of patients with persistent AF (PeAF) or both PAF/PeAF. Intermittent monitoring was associated with detection of significantly less atrial arrhythmia recurrence than continuous monitoring in PAF arms (31.2% vs 46.9%, P = 0.001), but not in PeAF/PAF-PeAF combined arms (43.3% vs 63.6%, P = 0.12). No significant relationship was seen between the duration of intermittent rhythm monitoring and atrial arrhythmia recurrence detection in either the PAF (P = 0.93) or PeAF/PAF-PeAF combined arms (P = 0.20).
Conclusions: Continuous rhythm monitoring detected higher atrial arrhythmia recurrence rates, compared to intermittent rhythm monitoring, in patients with PAF. The duration of intermittent monitoring did not show a statistically significant relationship to the yield of arrhythmia detection, in near identical cohorts of trial subjects undergoing similar interventions, with clinical and research implications.
Contexte: La stratégie qui consiste à surveiller le rythme cardiaque après une ablation par cathéter dans le traitement de la fibrillation auriculaire (FA) a un effet sur la détection de récidive de l’arythmie auriculaire, mais elle n’est pas bien définie. Nous avons mené une revue systématique et une méta-régression pour déterminer si le mode employé pour surveiller le rythme après une ablation par cathéter et la durée de cette surveillance ont un effet sur la détection de récidive de l’arythmie auriculaire.
Méthodologie: Des bases de données ont été systématiquement épluchées à la recherche d’essais contrôlés randomisés menés auprès d’adultes subissant leur première ablation par cathéter pour une FA entre 2007 et 2021. La durée et la stratégie utilisées dans la surveillance du rythme ont été recensées. La méta-régression a été utilisée pour déceler tout lien entre la durée de la surveillance et la détection d’une récidive de l’arythmie auriculaire. Le paramètre d’évaluation principal était la récidive de l’arythmie auriculaire avec une seule intervention.
Résultats: La stratégie de recherche a fait ressortir 57 groupes de 56 essais contrôlés randomisés comprenant 5 322 patients : 36 groupes de patients présentant une FA paroxystique et 21 groupes de patients présentant une FA persistante ou ces deux types de FA (paroxystique et persistante). La surveillance intermittente a été associée à une moins grande détection de cas d’arythmie auriculaire récidivante, comparativement à la surveillance constante (31,2 % vs 46,9 %, p = 0,001), ce qui n’a pas été le cas dans les groupes où les types de FA (persistante ou paroxystique et persistante) étaient combinés (43,3 % vs 63,6 %, p = 0,12). Aucun lien notable n’a été observé entre la durée de la surveillance intermittente du rythme et la détection de l’arythmie auriculaire récidivante dans le groupe FA paroxystique (p = 0,93) ou dans le groupe des types de FA combinés (p = 0,20).
Conclusions: Le taux de détection de l’arythmie auriculaire récidivante était plus élevé avec la surveillance constante qu’avec la surveillance intermittente chez les patients atteints de FA paroxystique. La durée de la surveillance intermittente n’a pas eu de lien statistiquement significatif avec le rendement de détection de l’arythmie, dans des cohortes presque identiques de participants aux essais subissant des interventions similaires, comportant des implications cliniques ou expérimentales.
© 2022 The Authors.
Figures
References
-
- January C.T., Wann L.S., Alpert J.S., et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64:e1–76. - PubMed
-
- European Heart Rhythm Association, European Association for Cardio-Thoracic Surgery. Camm A.J., et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Eur Heart J. 2010;31:2369–2429. - PubMed
-
- Lloyd-Jones D.M., Wang T.J., Leip E.P., et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation. 2004;110:1042–1046. - PubMed
-
- Wolf P.A., Mitchell J.B., Baker C.S., Kannel W.B., D'Agostino R.B. Impact of atrial fibrillation on mortality, stroke, and medical costs. Arch Intern Med. 1998;158:229–234. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
