

A Carotid Body Tumour Mimicking Richter's Transformation of Chronic Lymphocytic Leukaemia
- PMID: 35607576
- PMCID: PMC9123347
- DOI: 10.7759/cureus.24262
A Carotid Body Tumour Mimicking Richter's Transformation of Chronic Lymphocytic Leukaemia
Abstract
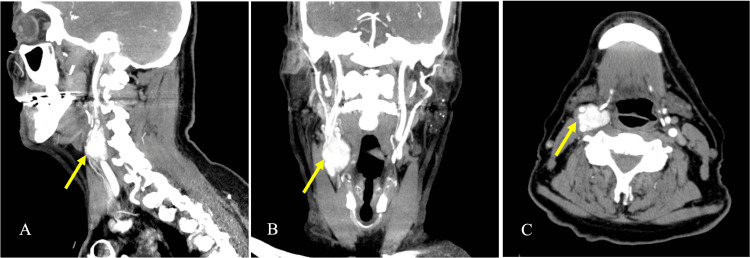
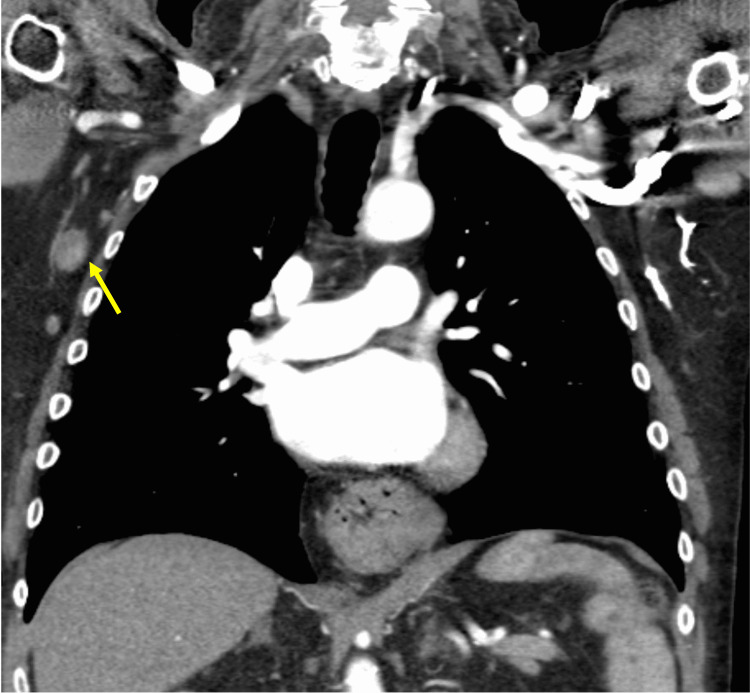
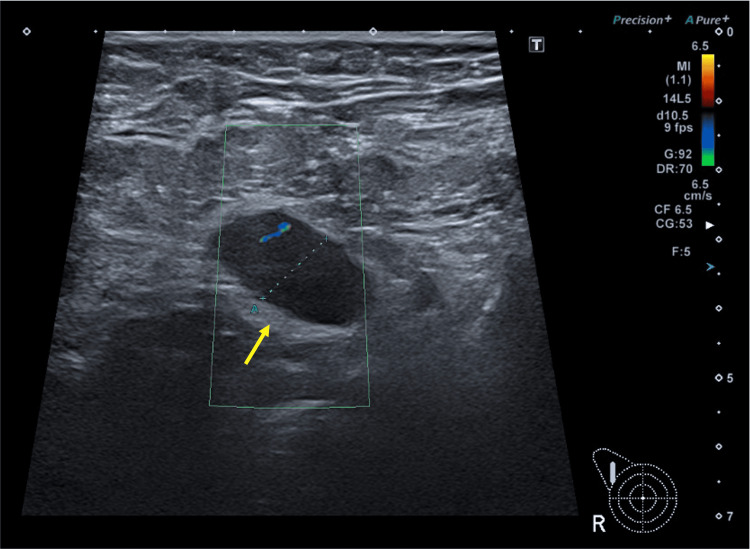
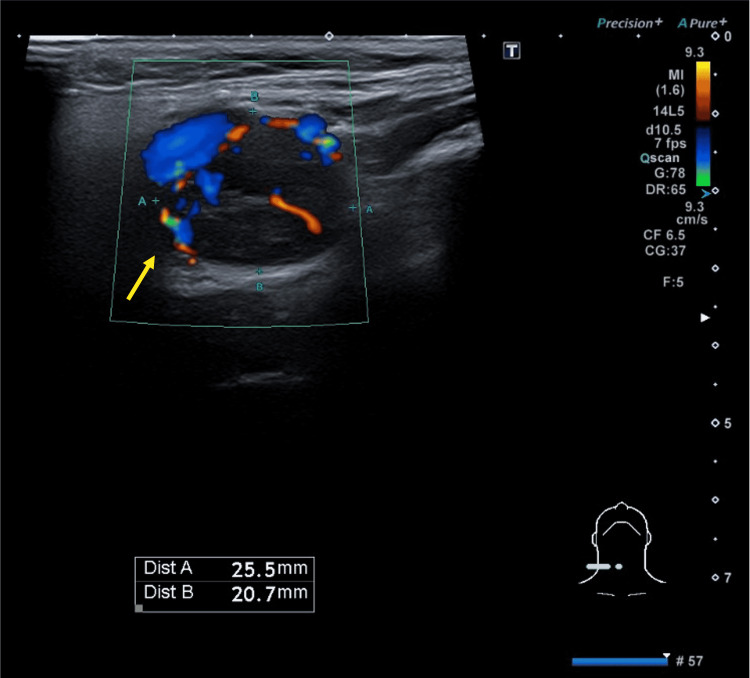
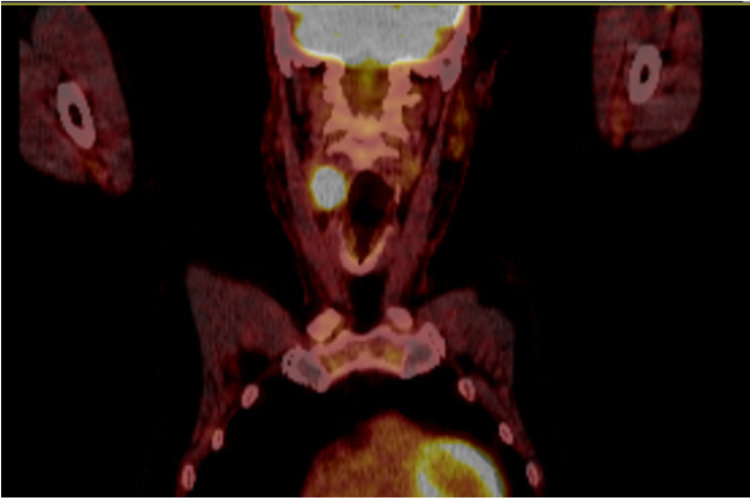
Carotid body tumours (CBT), also called carotid paragangliomas, are highly vascular glomus tumours that originate from paraganglionic cells of the carotid body. They are frequently asymptomatic, insidious, and non-secretory in nature. They typically present as a large, non-tender, pulsatile neck mass. Careful evaluation of a neck mass, with the aid of imaging, is necessary to avoid a misdiagnosis. We herein describe a case of a 77-year-old gentleman with a background of chronic B-cell lymphocytic leukaemia, who was found to have a rapidly enlarging, asymptomatic neck mass along with multiple enlarged lymph nodes in the axillae. Given his past medical history, the preliminary diagnosis was Richter's transformation. However, the characteristic splaying of the internal and external carotid arteries on imaging prompted us to consider the diagnosis of a CBT. The patient was referred to vascular surgeons for surgical excision of the tumour. Histology confirmed that the neck mass was indeed a CBT. Ultrasound-guided core biopsy of the axillary lymph nodes revealed a concomitant Hodgkin-like Richter's transformation. This case exemplifies how we were able to differentiate between a CBT and nodal mass with the aid of various imaging modalities. An accurate diagnosis allows clinicians to deliver the appropriate management; the treatment for CBT is surgical excision, whereas chemotherapy is the first-line treatment for Richter's transformation.
Keywords: carotid body tumour; carotid paraganglioma; chemodectoma; fontaine sign; head and neck tumors; lyre sign; non‑functional paraganglioma; richter’s transformation; shamblin; b-cell lymphoma.
Copyright © 2022, Qamar et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Detection of Richter's transformation of chronic lymphocytic leukemia by PET/CT.J Nucl Med. 2006 Aug;47(8):1267-73. J Nucl Med. 2006. PMID: 16883004
-
Hodgkin's disease variant of Richter's syndrome. Report of a case with diagnosis by fine needle biopsy.Acta Cytol. 1997 May-Jun;41(3):823-9. doi: 10.1159/000332710. Acta Cytol. 1997. PMID: 9167708
-
Microsatellite instability and hMLH1 promoter hypermethylation in Richter's transformation of chronic lymphocytic leukemia.Leukemia. 2003 Feb;17(2):411-5. doi: 10.1038/sj.leu.2402792. Leukemia. 2003. PMID: 12592341
-
Coexistence of chronic myeloid leukemia and diffuse large B-cell lymphoma with antecedent chronic lymphocytic leukemia: a case report and review of the literature.J Med Case Rep. 2018 Mar 11;12(1):64. doi: 10.1186/s13256-018-1612-4. J Med Case Rep. 2018. PMID: 29524963 Free PMC article. Review.
-
Richter's syndrome: biology and therapy.Cancer J. 2005 May-Jun;11(3):161-74. doi: 10.1097/00130404-200505000-00001. Cancer J. 2005. PMID: 16053658 Review.
References
-
- Combined endovascular and surgical treatment of head and neck paragangliomas—a team approach. Persky MS, Setton A, Niimi Y, Hartman J, Frank D, Berenstein A. Head Neck. 2002;24:423–431. - PubMed
-
- Paragangliomas of the head and neck: diagnosis and treatment. Boedeker CC, Ridder GJ, Schipper J. Fam Cancer. 2005;4:55–59. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous