

Comparison of ultra-low, low and high concentration local anaesthetic for labour epidural analgesia: a systematic review and network meta-analysis
- PMID: 35607864
- PMCID: PMC9543867
- DOI: 10.1111/anae.15756
Comparison of ultra-low, low and high concentration local anaesthetic for labour epidural analgesia: a systematic review and network meta-analysis
Abstract
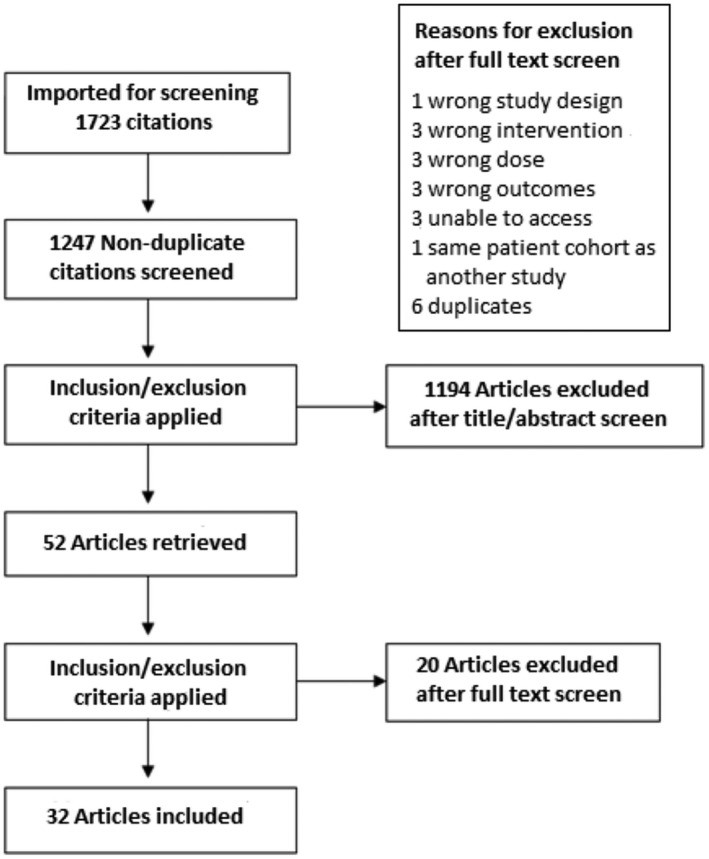
Lumbar epidural is the gold standard for labour analgesia. Low concentrations of local anaesthetic are recommended. This network meta-analysis investigated whether further reducing the concentration of local anaesthetic can improve maternal and neonatal outcomes without compromising analgesia. We conducted a systematic search of relevant databases for randomised controlled trials comparing high (>0.1%), low (>0.08% to ≤0.1%) or ultra-low (≤0.08%) concentration local anaesthetic (bupivacaine or equivalent) for labour epidural. Outcomes included mode of delivery, duration of labour and maternal/neonatal outcomes. Bayesian network meta-analysis with random-effects modelling was used to calculate odds ratios or weighted mean differences and 95% credible intervals. A total of 32 studies met inclusion criteria (3665 women). The total dose of local anaesthetic received increased as the concentration increased; ultra-low compared with low (weighted mean difference -14.96 mg, 95% credible interval [-28.38 to -1.00]) and low compared with high groups (weighted mean difference -14.99 [-28.79 to -2.04]), though there was no difference in the number of rescue top-ups administered between the groups. Compared with high concentration, ultra-low concentration local anaesthetic was associated with increased likelihood of spontaneous vaginal delivery (OR 1.46 [1.18 to 1.86]), reduced motor block (Bromage score >0; OR 0.32 [0.18 to 0.54]) and reduced duration of second stage of labour (weighted mean difference -13.02 min [-21.54 to -4.77]). Compared with low, ultra-low concentration local anaesthetic had similar estimates for duration of second stage of labour (weighted mean difference -1.92 min [-14.35 to 10.20]); spontaneous vaginal delivery (OR 1.07 [0.75 to 1.56]; assisted vaginal delivery (OR 1.35 [0.75 to 2.26]); caesarean section (OR 0.76 [0.49 to 1.22]); pain (scale 1-100, weighted mean difference -5.44 [-16.75 to 5.93]); and maternal satisfaction. Although a lower risk of an Apgar score < 7 at 1 min (OR 0.43 [0.15 to 0.79]) was reported for ultra-low compared with low concentration, this was not sustained at 5 min (OR 0.12 [0.00 to 2.10]). Ultra-low concentration local anaesthetic for labour epidural achieves similar or better maternal and neonatal outcomes as low and high concentration, but with reduced local anaesthetic consumption.
Keywords: Bayesian; epidural; labour analgesia; local anaesthetic; maternal outcomes; meta-analysis; obstetric outcomes.
© 2022 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists.
Figures


References
-
- Vedagiri Sai R, Rappai G, Johnstone C. Survey of obstetric epidural anaesthetic practises in Scotland. Abstract presented at the Obstetric Anaesthetists' Association Annual Meeting, Bournemouth, 2013: 43. https://www.oaa-anaes.ac.uk/assets/_managed/editor/File/Courses/2013/13.... (accessed 27/04/2022).
-
- Sultan P, Murphy C, Halpern S, Carvalho B. The effect of low concentrations versus high concentrations of local anesthetics for labour analgesia on obstetric and anesthetic outcomes: a meta‐analysis. Canadian Journal of Anesthesia 2013; 60: 840–54. - PubMed
