

Artificial Intelligence Tool for Assessment of Indeterminate Pulmonary Nodules Detected with CT
- PMID: 35608444
- PMCID: PMC9434821
- DOI: 10.1148/radiol.212182
Artificial Intelligence Tool for Assessment of Indeterminate Pulmonary Nodules Detected with CT
Abstract
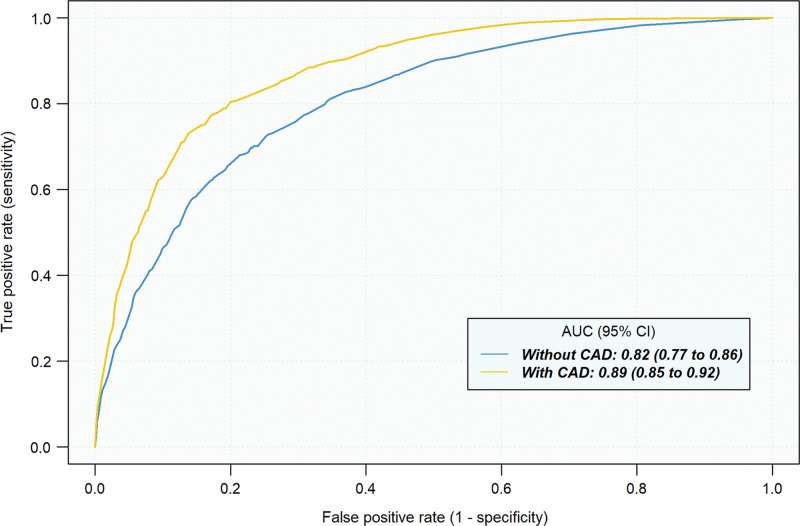
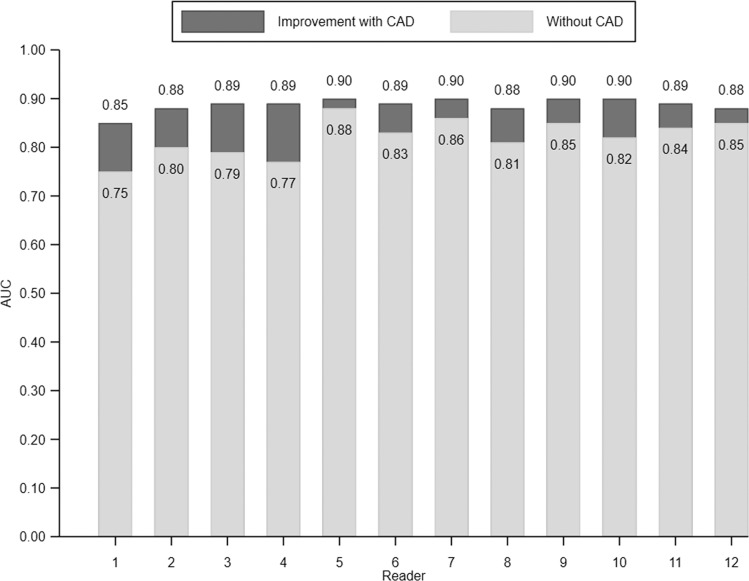
Background Limited data are available regarding whether computer-aided diagnosis (CAD) improves assessment of malignancy risk in indeterminate pulmonary nodules (IPNs). Purpose To evaluate the effect of an artificial intelligence-based CAD tool on clinician IPN diagnostic performance and agreement for both malignancy risk categories and management recommendations. Materials and Methods This was a retrospective multireader multicase study performed in June and July 2020 on chest CT studies of IPNs. Readers used only CT imaging data and provided an estimate of malignancy risk and a management recommendation for each case without and with CAD. The effect of CAD on average reader diagnostic performance was assessed using the Obuchowski-Rockette and Dorfman-Berbaum-Metz method to calculate estimates of area under the receiver operating characteristic curve (AUC), sensitivity, and specificity. Multirater Fleiss κ statistics were used to measure interobserver agreement for malignancy risk and management recommendations. Results A total of 300 chest CT scans of IPNs with maximal diameters of 5-30 mm (50.0% malignant) were reviewed by 12 readers (six radiologists, six pulmonologists) (patient median age, 65 years; IQR, 59-71 years; 164 [55%] men). Readers' average AUC improved from 0.82 to 0.89 with CAD (P < .001). At malignancy risk thresholds of 5% and 65%, use of CAD improved average sensitivity from 94.1% to 97.9% (P = .01) and from 52.6% to 63.1% (P < .001), respectively. Average reader specificity improved from 37.4% to 42.3% (P = .03) and from 87.3% to 89.9% (P = .05), respectively. Reader interobserver agreement improved with CAD for both the less than 5% (Fleiss κ, 0.50 vs 0.71; P < .001) and more than 65% (Fleiss κ, 0.54 vs 0.71; P < .001) malignancy risk categories. Overall reader interobserver agreement for management recommendation categories (no action, CT surveillance, diagnostic procedure) also improved with CAD (Fleiss κ, 0.44 vs 0.52; P = .001). Conclusion Use of computer-aided diagnosis improved estimation of indeterminate pulmonary nodule malignancy risk on chest CT scans and improved interobserver agreement for both risk stratification and management recommendations. © RSNA, 2022 Online supplemental material is available for this article. See also the editorial by Yanagawa in this issue.
Conflict of interest statement
Figures



![Reclassification plots with and without computer-aided diagnosis (CAD)
for malignant and benign pulmonary nodules. Summary plots of all pairs of
pre-CAD (x-axis) and post-CAD (y-axis) malignancy risk estimates for
malignant (n = 1800 [150 cases × 12 readers]) (A) and benign (n =
1800 [150 cases × 12 readers]) (B) nodules. Malignancy risk decision
thresholds of 5% and 65% are depicted as gray lines in each plot.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/2a72/9434821/cf20281586bc/radiol.212182.fig6.jpg)
Comment in
-
Artificial Intelligence Improves Radiologist Performance for Predicting Malignancy at Chest CT.Radiology. 2022 Sep;304(3):692-693. doi: 10.1148/radiol.220571. Epub 2022 May 24. Radiology. 2022. PMID: 35608448 No abstract available.
References
-
- Gould MK , Donington J , Lynch WR , et al. . Evaluation of individuals with pulmonary nodules: when is it lung cancer? Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines . Chest 2013. ; 143 ( 5 Suppl):e93S – e120S. - PMC - PubMed
-
- Mazzone PJ , Lam L . Evaluating the Patient With a Pulmonary Nodule: A Review . JAMA 2022. ; 327 ( 3):264 – 273. - PubMed
-
- Gould MK , Tang T , Liu IL , et al. . Recent Trends in the Identification of Incidental Pulmonary Nodules . Am J Respir Crit Care Med 2015. ; 192 ( 10):1208 – 1214. - PubMed
-
- de Koning HJ , van der Aalst CM , de Jong PA , et al. . Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial . N Engl J Med 2020. ; 382 ( 6):503 – 513. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
