

Enhancement of cranial nerves in Lyme neuroborreliosis: incidence and correlation with clinical symptoms and prognosis
- PMID: 35608630
- PMCID: PMC9643208
- DOI: 10.1007/s00234-022-02957-2
Enhancement of cranial nerves in Lyme neuroborreliosis: incidence and correlation with clinical symptoms and prognosis
Abstract
Purpose: Symptoms of cranial neuritis are a common presentation of Lyme neuroborreliosis (LNB). Imaging studies are scarce and report contradictory low prevalence of enhancement compared to clinical studies of cranial neuropathy. We hypothesized that MRI enhancement of cranial nerves in LNB is underreported, and aimed to assess the prevalence and clinical impact of cranial nerve enhancement in early LNB.
Methods: In this prospective, longitudinal cohort study, 69 patients with acute LNB were examined with MRI of the brain. Enhancement of cranial nerves III-XII was rated. MRI enhancement was correlated to clinical findings of neuropathy in the acute phase and after 6 months.
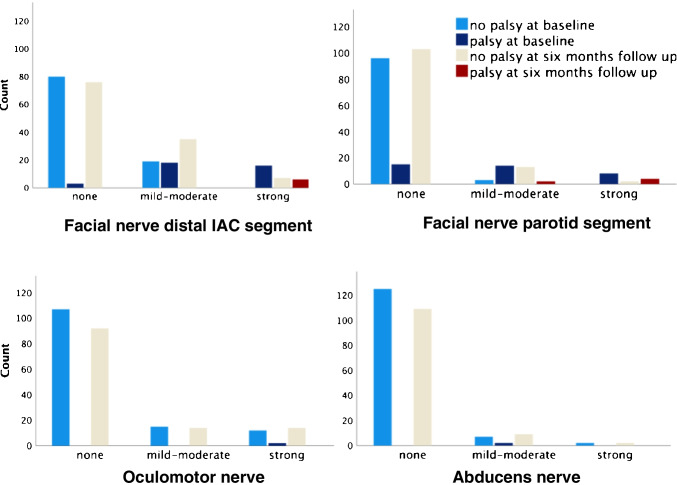
Results: Thirty-nine of 69 patients (57%) had pathological cranial nerve enhancement. Facial and oculomotor nerves were most frequently affected. There was a strong correlation between enhancement in the distal internal auditory canal and parotid segments of the facial nerve and degree of facial palsy (gamma = 0.95, p < .01, and gamma = 0.93, p < .01), despite that 19/37 nerves with mild-moderate enhancement in the distal internal auditory canal segment showed no clinically evident palsy. Oculomotor and abducens nerve enhancement did not correlate with eye movement palsy (gamma = 1.00 and 0.97, p = .31 for both). Sixteen of 17 patients with oculomotor and/or abducens nerve enhancement had no evident eye movement palsy.
Conclusions: MRI cranial nerve enhancement is common in LNB patients, but it can be clinically occult. Facial and oculomotor nerves are most often affected. Enhancement of the facial nerve distal internal auditory canal and parotid segments correlate with degree of facial palsy.
Keywords: Central nervous system infections; Cranial nerves; Lyme neuroborreliosis; Magnetic resonance imaging; Vector borne diseases.
© 2022. The Author(s).
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies: Mona K. Beyer received minor grants or speaker’s fees from Biogen Idec, Merck, and Novartis. Hanne F. Harbo received minor grants or speaker’s fees from Biogen, Sanofi Genzyme, Teva, and Merck. Åslaug R. Lorentzen received minor grant from Sanofi. The other authors do not report any disclosures.
Figures




References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
