

11C-methionine PET aids localization of microprolactinomas in patients with intolerance or resistance to dopamine agonist therapy
- PMID: 35608811
- PMCID: PMC9345820
- DOI: 10.1007/s11102-022-01229-9
11C-methionine PET aids localization of microprolactinomas in patients with intolerance or resistance to dopamine agonist therapy
Abstract
Purpose: To assess the potential for 11C-methionine PET (Met-PET) coregistered with volumetric magnetic resonance imaging (Met-PET/MRCR) to inform clinical decision making in patients with poorly visualized or occult microprolactinomas and dopamine agonist intolerance or resistance.
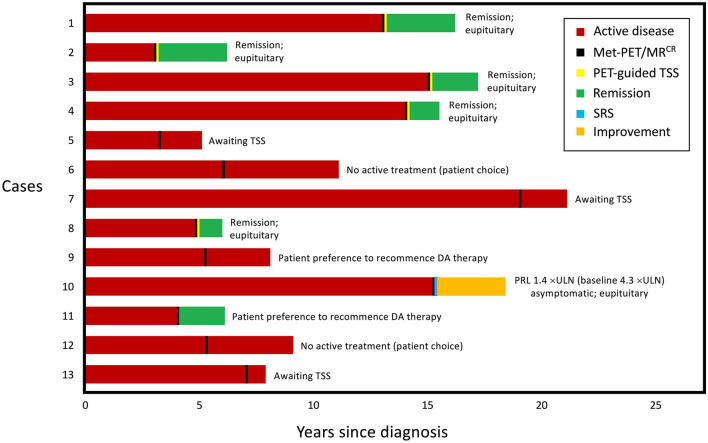
Patients and methods: Thirteen patients with pituitary microprolactinomas, and who were intolerant (n = 11) or resistant (n = 2) to dopamine agonist therapy, were referred to our specialist pituitary centre for Met-PET/MRCR between 2016 and 2020. All patients had persistent hyperprolactinemia and were being considered for surgical intervention, but standard clinical MRI had shown either no visible adenoma or equivocal appearances.
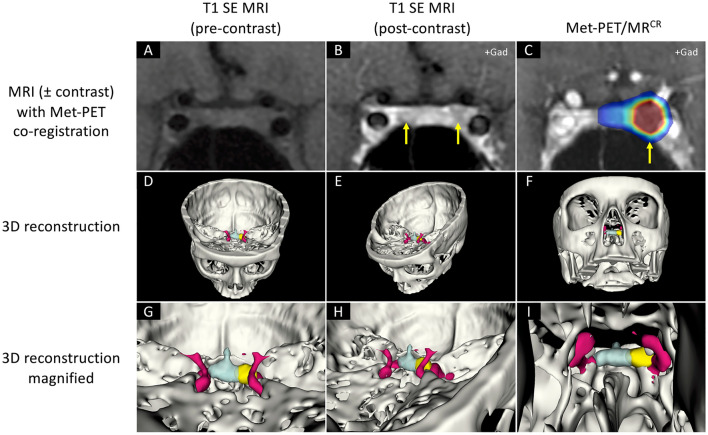
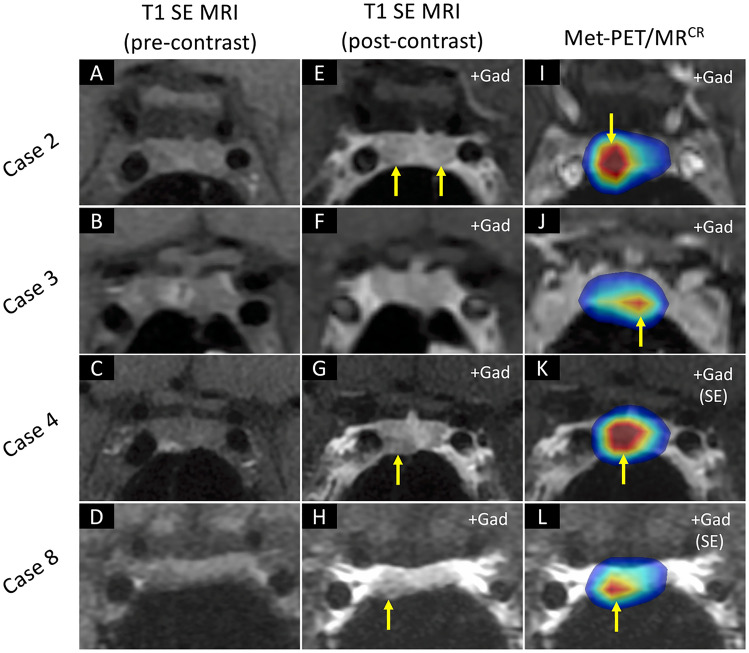
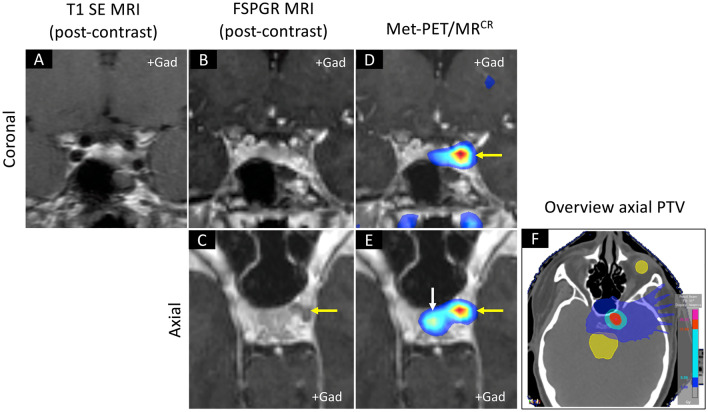
Results: In all 13 patients Met-PET/MRCR demonstrated a single focus of avid tracer uptake. This was localized either to the right or left side of the sella in 12 subjects. In one patient, who had previously undergone surgery for a left-sided adenoma, recurrent tumor was unexpectedly identified in the left cavernous sinus. Five patients underwent endoscopic transsphenoidal selective adenomectomy, with subsequent complete remission of hyperprolactinaemia and normalization of other pituitary function; three patients are awaiting surgery. In the patient with inoperable cavernous sinus disease PET-guided stereotactic radiosurgery (SRS) was performed with subsequent near-normalization of serum prolactin. Two patients elected for a further trial of medical therapy, while two declined surgery or radiotherapy and chose to remain off medical treatment.
Conclusions: In patients with dopamine agonist intolerance or resistance, and indeterminate pituitary MRI, molecular (functional) imaging with Met-PET/MRCR can allow precise localization of a microprolactinoma to facilitate selective surgical adenomectomy or SRS.
Keywords: 11C-methionine PET; Dopamine agonist intolerance/ resistance; Microprolactinoma.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Authors have no competing interests, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Figures
Similar articles
-
Implementation of functional imaging using 11C-methionine PET-CT co-registered with MRI for advanced surgical planning and decision making in prolactinoma surgery.Pituitary. 2022 Aug;25(4):587-601. doi: 10.1007/s11102-022-01230-2. Epub 2022 May 26. Pituitary. 2022. PMID: 35616762 Free PMC article.
-
Recurrence of hyperprolactinaemia following discontinuation of dopamine agonist therapy in patients with prolactinoma occurs commonly especially in macroprolactinoma.Clin Endocrinol (Oxf). 2011 Dec;75(6):819-24. doi: 10.1111/j.1365-2265.2011.04136.x. Clin Endocrinol (Oxf). 2011. PMID: 21645021
-
Endoscopic Transnasal Approach for Microprolactinomas with Experience of 105 Cases in a Single Center: Paradigmal Shift for Conventional Medical Therapy.World Neurosurg. 2023 Feb;170:e858-e867. doi: 10.1016/j.wneu.2022.12.003. Epub 2022 Dec 5. World Neurosurg. 2023. PMID: 36481446
-
Prolactinoma surgery.Ann Endocrinol (Paris). 2007 Jun;68(2-3):118-9. doi: 10.1016/j.ando.2007.03.011. Epub 2007 May 21. Ann Endocrinol (Paris). 2007. PMID: 17512893 Review.
-
Update on prolactinomas. Part 2: Treatment and management strategies.J Clin Neurosci. 2015 Oct;22(10):1568-74. doi: 10.1016/j.jocn.2015.03.059. Epub 2015 Aug 1. J Clin Neurosci. 2015. PMID: 26243714 Review.
Cited by
-
Clinical use of [18F]fluoro-ethyl-L-tyrosine PET co-registered with MRI for localizing prolactinoma remnants.Pituitary. 2024 Oct;27(5):614-624. doi: 10.1007/s11102-024-01430-y. Epub 2024 Jul 23. Pituitary. 2024. PMID: 39042164 Free PMC article.
-
Diagnosis and management of prolactin-secreting pituitary adenomas: a Pituitary Society international Consensus Statement.Nat Rev Endocrinol. 2023 Dec;19(12):722-740. doi: 10.1038/s41574-023-00886-5. Epub 2023 Sep 5. Nat Rev Endocrinol. 2023. PMID: 37670148 Review.
-
Development of a bespoke phantom to optimize molecular PET imaging of pituitary tumors.EJNMMI Phys. 2023 Jun 1;10(1):34. doi: 10.1186/s40658-023-00552-9. EJNMMI Phys. 2023. PMID: 37261547 Free PMC article.
-
The Use of [11C]C-Methionine in Diagnostics of Endocrine Disorders with Focus on Pituitary and Parathyroid Glands.Pharmaceuticals (Basel). 2025 Feb 7;18(2):229. doi: 10.3390/ph18020229. Pharmaceuticals (Basel). 2025. PMID: 40006042 Free PMC article. Review.
-
The Changing Treatment Paradigm for Prolactinoma-A Prospective Series of 100 Consecutive Neurosurgical Cases.J Clin Endocrinol Metab. 2025 May 19;110(6):e1833-e1844. doi: 10.1210/clinem/dgae652. J Clin Endocrinol Metab. 2025. PMID: 39292628 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
