

Making sense of phantom limb pain
- PMID: 35609964
- PMCID: PMC9304093
- DOI: 10.1136/jnnp-2021-328428
Making sense of phantom limb pain
Abstract
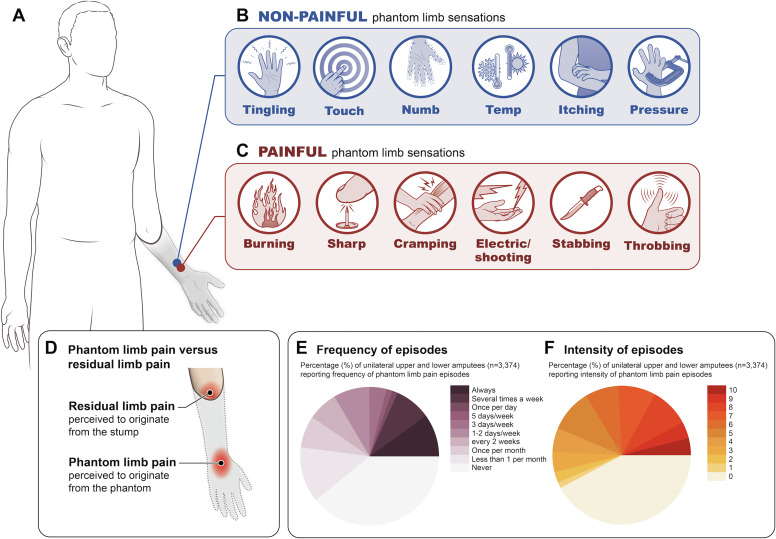
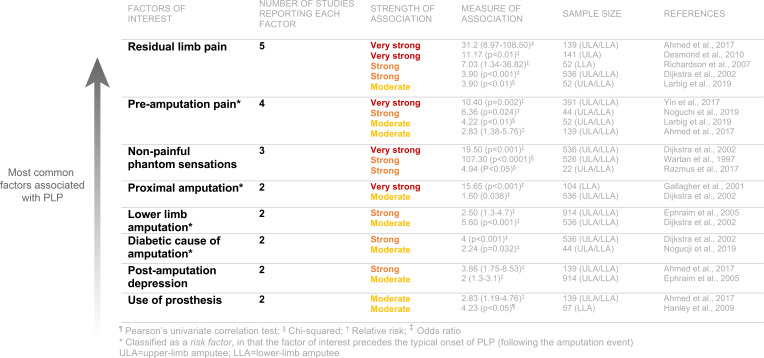
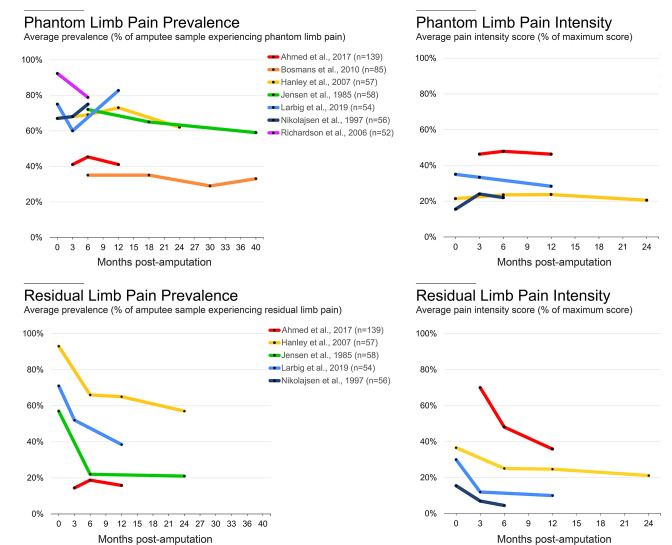
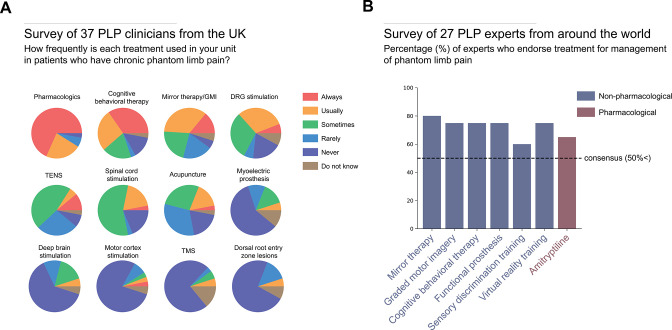
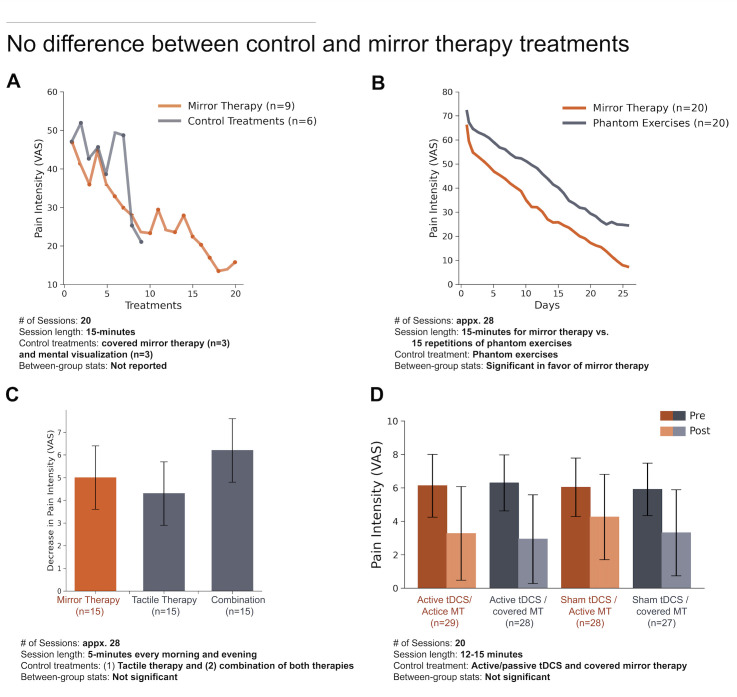
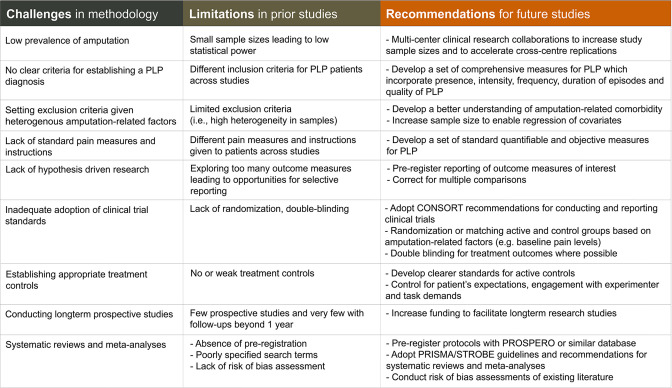
Phantom limb pain (PLP) impacts the majority of individuals who undergo limb amputation. The PLP experience is highly heterogenous in its quality, intensity, frequency and severity. This heterogeneity, combined with the low prevalence of amputation in the general population, has made it difficult to accumulate reliable data on PLP. Consequently, we lack consensus on PLP mechanisms, as well as effective treatment options. However, the wealth of new PLP research, over the past decade, provides a unique opportunity to re-evaluate some of the core assumptions underlying what we know about PLP and the rationale behind PLP treatments. The goal of this review is to help generate consensus in the field on how best to research PLP, from phenomenology to treatment. We highlight conceptual and methodological challenges in studying PLP, which have hindered progress on the topic and spawned disagreement in the field, and offer potential solutions to overcome these challenges. Our hope is that a constructive evaluation of the foundational knowledge underlying PLP research practices will enable more informed decisions when testing the efficacy of existing interventions and will guide the development of the next generation of PLP treatments.
Keywords: BRAIN MAPPING; COGNITION; MOTOR CONTROL; PAIN; SOMATISATION DISORDER.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous