

Postinjury complement C4 activation is associated with adverse outcomes and is potentially influenced by plasma resuscitation
- PMID: 35610738
- PMCID: PMC9613483
- DOI: 10.1097/TA.0000000000003713
Postinjury complement C4 activation is associated with adverse outcomes and is potentially influenced by plasma resuscitation
Abstract
Background: Complement activation after trauma promotes hemostasis but is associated with increased morbidity and mortality. However, the specific pathways and downstream mediators remain unclear. Recently, the anaphylatoxin C4a has been shown to bind to thrombin receptors. While plasma-based resuscitation has been shown to modify the endotheliopathy of trauma, it may provide complement zymogens that fuel ongoing inflammatory cascades. We sought to characterize the activation of complement after injury and the effect of fresh frozen plasma (FFP) on this inflammatory response. We hypothesized that trauma induces C4 activation, which is associated with worse outcomes and influenced by FFP resuscitation.
Methods: Blood was collected from injured patients at a single level I trauma center enrolled in the Control of Major Bleeding after Trauma (COMBAT) randomized clinical trial. Proteomic analyses were performed through targeted liquid chromatography coupled with mass spectrometry. For the present observational study, concentrations of complement proteins were analyzed at multiple time points, compared between treatment groups, and correlated with outcomes.
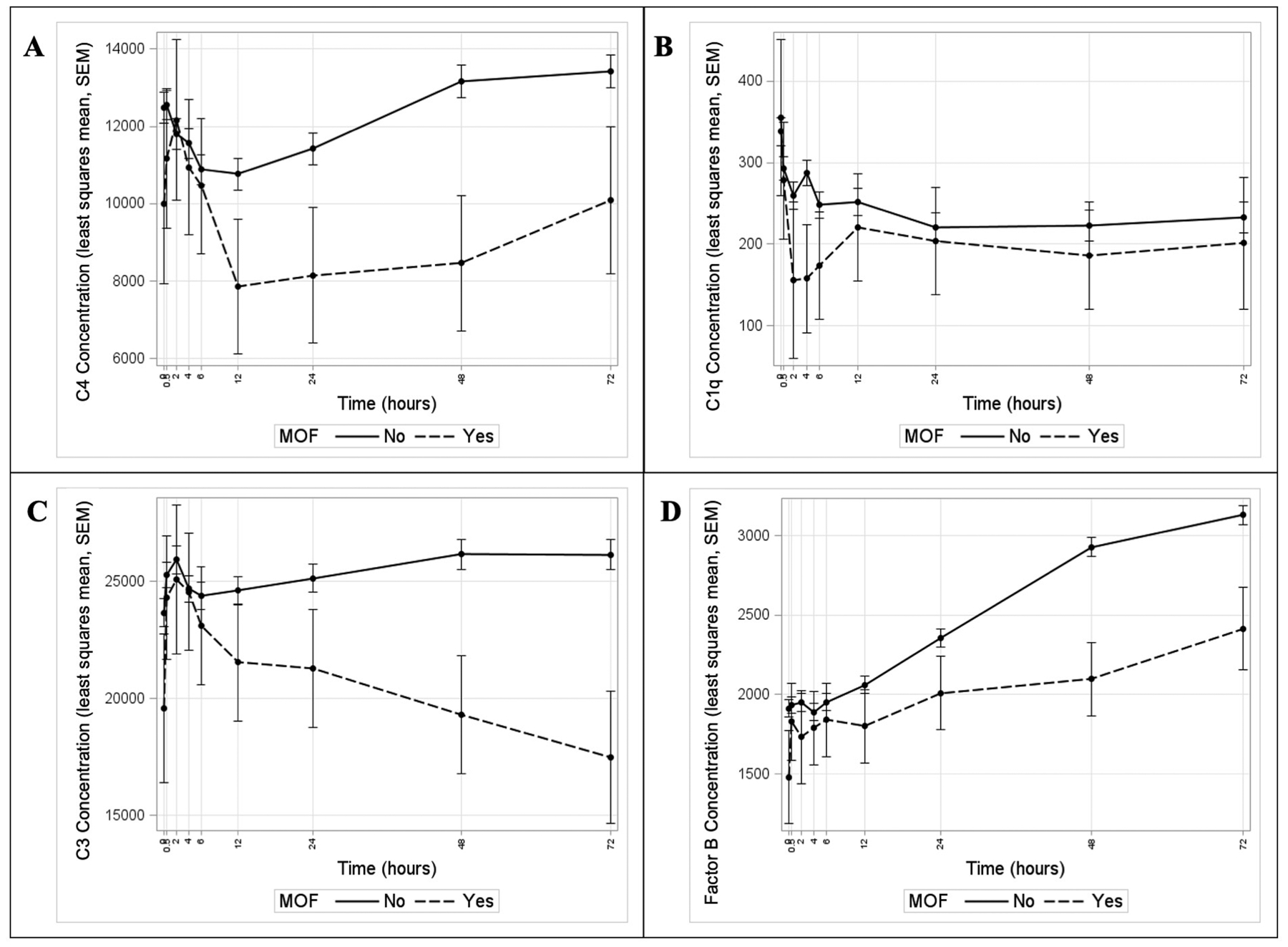
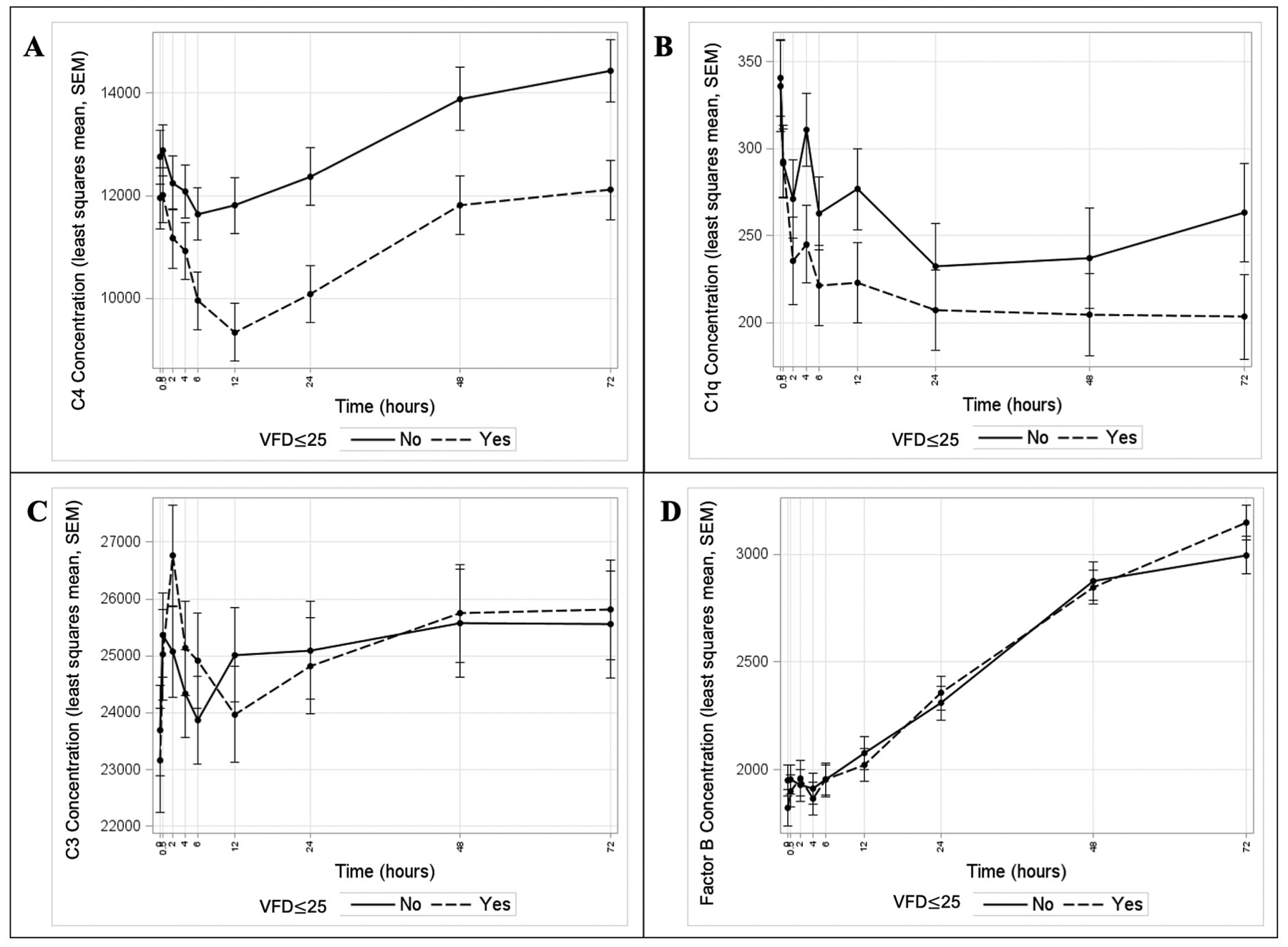
Results: C4 activation occurred over the first 6 hours postinjury with peak activation 6 to 24 hours. Tissue hypoperfusion, defined as base deficit >10 mEq/L, and requirement for massive transfusion were associated with greater C4 activation. C4 activation was associated with mortality, multiple organ failure, and longer ventilator requirement. In addition, temporal trends of C1q, factor B, and C3 by outcome groups support the prevailing theory of primary classical pathway activation with alternative pathway amplification. Resuscitation with FFP over the first 6 hours was associated with increased C4 activation at 12 and 24 hours.
Conclusion: C4 activation has an important inflammatory role postinjury, and FFP has the potential to augment this complement activation during resuscitation.
Level of evidence: Prognostic/epidemiological, level III.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Figures



References
-
- Ganter MT, Brohi K, Cohen MJ, Shaffer LA, Walsh MC, Stahl GL, et al. Role of the alternative pathway in the early complement activation following major trauma. Shock. 2007;28(1):29–34 - PubMed
-
- Stahel PF, Smith WR, Moore EE. Role of biological modifiers regulating the immune response after trauma. Injury. 2007;38(12):1409–22 - PubMed
-
- Thurman JM, Holers VM. The central role of the alternative complement pathway in human disease. J Immunol. 2006;176(3):1305–10 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
