

Predictors of all-cause mortality among patients hospitalized with influenza, respiratory syncytial virus, or SARS-CoV-2
- PMID: 35611399
- PMCID: PMC9347457
- DOI: 10.1111/irv.13004
Predictors of all-cause mortality among patients hospitalized with influenza, respiratory syncytial virus, or SARS-CoV-2
Abstract
Background: Shared and divergent predictors of clinical severity across respiratory viruses may support clinical and community responses in the context of a novel respiratory pathogen.
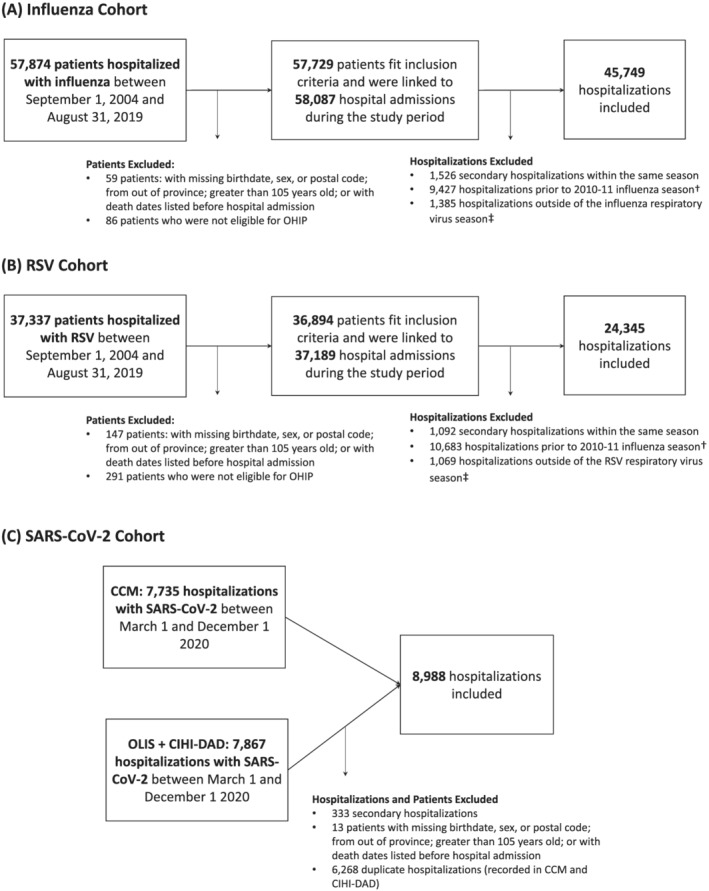
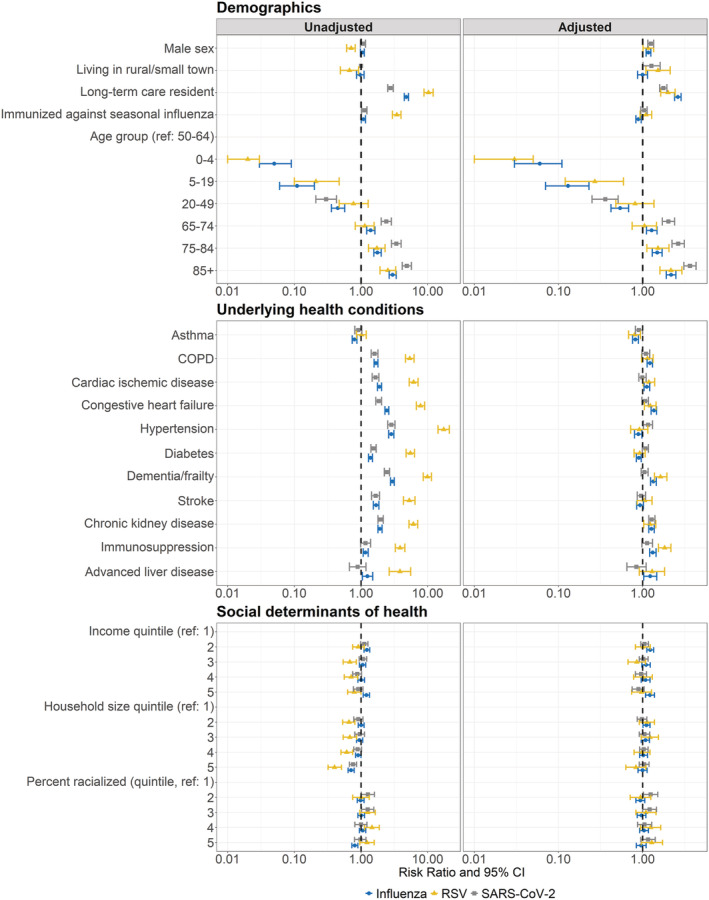
Methods: We conducted a retrospective cohort study to identify predictors of 30-day all-cause mortality following hospitalization with influenza (N = 45,749; 2010-09 to 2019-05), respiratory syncytial virus (RSV; N = 24 345; 2010-09 to 2019-04), or severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; N = 8988; 2020-03 to 2020-12; pre-vaccine) using population-based health administrative data from Ontario, Canada. Multivariable modified Poisson regression was used to assess associations between potential predictors and mortality. We compared the direction, magnitude, and confidence intervals of risk ratios to identify shared and divergent predictors of mortality.
Results: A total of 3186 (7.0%), 697 (2.9%), and 1880 (20.9%) patients died within 30 days of hospital admission with influenza, RSV, and SARS-CoV-2, respectively. Shared predictors of increased mortality included older age, male sex, residence in a long-term care home, and chronic kidney disease. Positive associations between age and mortality were largest for patients with SARS-CoV-2. Few comorbidities were associated with mortality among patients with SARS-CoV-2 as compared with those with influenza or RSV.
Conclusions: Our findings may help identify patients at greatest risk of illness secondary to a respiratory virus, anticipate hospital resource needs, and prioritize local prevention and therapeutic strategies to communities with higher prevalence of risk factors.
Keywords: SARS-CoV-2; hospitalization; influenza; mortality; respiratory syncytial virus.
© 2022 The Authors. Influenza and Other Respiratory Viruses published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no competing interests that are relevant to the content of this article.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
