

Empagliflozin reduces markers of acute kidney injury in patients with acute decompensated heart failure
- PMID: 35611683
- PMCID: PMC9288802
- DOI: 10.1002/ehf2.13955
Empagliflozin reduces markers of acute kidney injury in patients with acute decompensated heart failure
Abstract
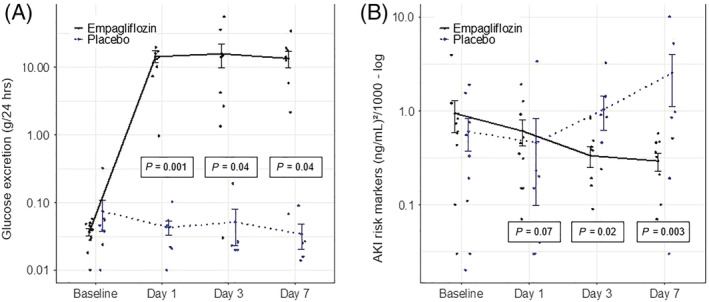
Aims: In this prospective, placebo-controlled, double-blind, exploratory study, we examined early and more delayed effects of empagliflozin treatment on haemodynamic parameters (primary endpoint: cardiac output) and kidney function including parameters of acute kidney injury (AKI) in patients with acute decompensated heart failure (HF).
Methods and results: Patients with acute decompensated HF with or without diabetes were randomized to empagliflozin 10 mg or placebo for 30 days. Haemodynamic, laboratory, and urinary parameters were assessed after 6 h, 1 day, 3 days, 7 days, and 30 days of treatment. Median time between hospital admission and randomization was 72 h. Baseline characteristics were not different in the empagliflozin (n = 10) and placebo (n = 9) groups. Empagliflozin led to a significant increase in urinary glucose excretion throughout the study (baseline: 37 ± 15 mg/24 h; Day 1: 14 565 ± 8663 mg/24 h; P = 0.001). Empagliflozin did not affect the primary endpoint of cardiac index or on systemic vascular resistance index at any time point. However, empagliflozin significantly reduced parameters of AKI (urinary TIMP-2 and IGFBP7 by NephroCheck® as indicators of tubular kidney damage), which became significant after 3 days of treatment [placebo: 1.1 ± 1.1 (ng/mL)2 /1000; empagliflozin: 0.3 ± 0.2 (ng/mL)2 /1000; P = 0.02] and remained significant at the 7 day time point [placebo: 2.5 ± 3.8 (ng/mL)2 /1000; empagliflozin: 0.3 ± 0.2 (ng/mL)2 /1000; P = 0.003].
Conclusions: In this study, empagliflozin treatment did not affect haemodynamic parameters but significantly reduced markers of tubular injury in patients with acute decompensated HF.
Keywords: Acute decompensated heart failure; Acute kidney injury; Empagliflozin; Haemodynamic parameters; SGLT2 inhibitors.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
K.T., M.R., N.U.K.H., M.M., J.M., and A.K. report no potential conflict of interest. J.J. has given lectures for Bayer and Fresenius Medica Care. In addition, he holds four patents in the topic of the manuscript and is inventor of an additional, already sold patent to Baxter. M.B. received speaker honoraria from Astra‐Zeneca and Boehringer Ingelheim and was national coordinator of DAPA‐HF and EMPEROR‐Reduced. J.F. has received consultancy fees from AstraZeneca, Bayer, Boehringer, and Vifor and is a member of the data safety monitoring committee in NovoNordisk trials. N.M. has received support for clinical trial leadership from Boehringer Ingelheim and Novo Nordisk and served as a consultant to Boehringer Ingelheim, Merck, Novo Nordisk, and AstraZeneca. B.M.S. received grant support from Boehringer Ingelheim, Merck, and Novo Nordisk and served as a speaker for Boehringer Ingelheim, Merck, Novo Nordisk, Lilly, BMS, and Astra Zeneca. M.L. received grants and personal fees from Boehringer Ingelheim, MSD, and Novo Nordisk and personal fees from Amgen, Sanofi, Astra Zeneca, Bayer, and Lilly.
Figures
References
-
- Bubenek‐Turconi SI, Craciun M, Miclea I, Perel A. Noninvasive continuous cardiac output by the Nexfin before and after preload‐modifying maneuvers: a comparison with intermittent thermodilution cardiac output. Anesth Analg. 2013; 117: 366–372. - PubMed
-
- Broch O, Renner J, Gruenewald M, Meybohm P, Schöttler J, Caliebe A, Steinfath M, Malbrain M, Bein B. A comparison of the Nexfin® and transcardiopulmonary thermodilution to estimate cardiac output during coronary artery surgery. Anaesthesia. 2012; 67: 377–383. - PubMed
-
- Filippatos G, Farmakis D, Parissis J. Renal dysfunction and heart failure: things are seldom what they seem. Eur Heart J. 2014; 35: 416–418. - PubMed
-
- Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, Januzzi J, Verma S, Tsutsui H, Brueckmann M, Jamal W, Kimura K, Schnee J, Zeller C, Cotton D, Bocchi E, Böhm M, Choi DJ, Chopra V, Chuquiure E, Giannetti N, Janssens S, Zhang J, Gonzalez Juanatey JR, Kaul S, Brunner‐la Rocca HP, Merkely B, Nicholls SJ, Perrone S, Pina I, Ponikowski P, Sattar N, Senni M, Seronde MF, Spinar J, Squire I, Taddei S, Wanner C, Zannad F. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020; 383: 1413–1424. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous