

An update on polymyalgia rheumatica
- PMID: 35612524
- PMCID: PMC9796644
- DOI: 10.1111/joim.13525
An update on polymyalgia rheumatica
Abstract
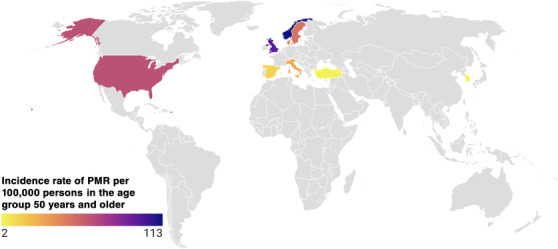
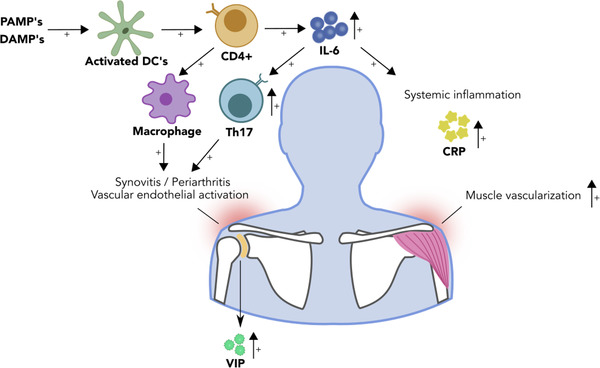
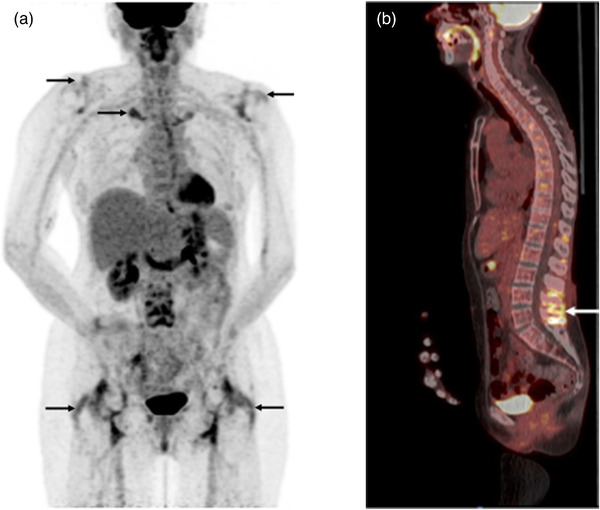
Polymyalgia rheumatica (PMR) is the most common inflammatory rheumatic disease affecting people older than 50 years and is 2-3 times more common in women. The most common symptoms are pain and morning stiffness in the shoulder and pelvic girdle and the onset may be acute or develop over a few days to weeks. General symptoms such as fatigue, fever and weight loss may occur, likely driven by systemic IL-6 signalling. The pathology includes synovial and periarticular inflammation and muscular vasculopathy. A new observation is that PMR may appear as a side effect of cancer treatment with checkpoint inhibitors. The diagnosis of PMR relies mainly on symptoms and signs combined with laboratory markers of inflammation. Imaging modalities including ultrasound, magnetic resonance imaging and positron emission tomography with computed tomography are promising new tools in the investigation of suspected PMR. However, they are still limited by availability, high cost and unclear performance in the diagnostic workup. Glucocorticoid (GC) therapy is effective in PMR, with most patients responding promptly to 15-25 mg prednisolone per day. There are challenges in the management of patients with PMR as relapses do occur and patients with PMR may need to stay on GC for extended periods. This is associated with high rates of GC-related comorbidities, such as diabetes and osteoporosis, and there are limited data on the use of disease-modifying antirheumatic drugs and biologics as GC sparing agents. Finally, PMR is associated with giant cell arteritis that may complicate the disease course and require more intense and prolonged treatment.
Keywords: diagnosis; epidemiology; giant cell arteritis; polymyalgia rheumatica; temporal arteritis; treatment.
© 2022 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
Ingrid E. Lundberg has stock shares in Roche and Novartis. Carl Turesson has received honoraria for lectures and educational events from Abbvie, Bristol‐Myers Squibb, Nordic Drugs, Pfizer and Roche. Aladdin J. Mohammad has received honoraria for lectures and educational events from Roche, GSK, Vifor, Lilly and AMGEN.
Figures
References
-
- Doran MF, Crowson CS, O'Fallon WM, Hunder GG, Gabriel SE. Trends in the incidence of polymyalgia rheumatica over a 30 year period in Olmsted County, Minnesota, USA. J Rheumatol. 2002;29:1694–7. - PubMed
-
- Gonzalez‐Gay MA, Vazquez‐Rodriguez TR, Lopez‐Diaz MJ, Miranda‐Filloy JA, Gonzalez‐Juanatey C, Martin J, et al. Epidemiology of giant cell arteritis and polymyalgia rheumatica. Arthritis Rheum. 2009;61:1454–61. - PubMed
-
- Noltorp S, Svensson B. High incidence of polymyalgia rheumatica and giant cell arteritis in a Swedish community. Clin Exp Rheumatol. 1991;9:351–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
