

Self-selection vs Randomized Assignment of Treatment for Appendicitis
- PMID: 35612859
- PMCID: PMC9134042
- DOI: 10.1001/jamasurg.2022.1554
Self-selection vs Randomized Assignment of Treatment for Appendicitis
Erratum in
-
Error in Figure and Results.JAMA Surg. 2022 Oct 1;157(10):971. doi: 10.1001/jamasurg.2022.4026. JAMA Surg. 2022. PMID: 35976664 Free PMC article. No abstract available.
Abstract
Importance: For adults with appendicitis, several randomized clinical trials have demonstrated that antibiotics are an effective alternative to appendectomy. However, it remains unknown how the characteristics of patients in such trials compare with those of patients who select their treatment and whether outcomes differ.
Objective: To compare participants in the Comparison of Outcomes of Antibiotic Drugs and Appendectomy (CODA) randomized clinical trial (RCT) with a parallel cohort study of participants who declined randomization and self-selected treatment.
Design, setting, and participants: The CODA trial was conducted in 25 US medical centers. Participants were enrolled between May 3, 2016, and February 5, 2020; all participants were eligible for at least 1 year of follow-up, with all follow-up ending in 2021. The randomized cohort included 1094 adults with appendicitis; the self-selection cohort included patients who declined participation in the randomized group, of whom 253 selected appendectomy and 257 selected antibiotics. In this secondary analysis, characteristics and outcomes in both self-selection and randomized cohorts are described with an exploratory analysis of cohort status and receipt of appendectomy.
Interventions: Appendectomy vs antibiotics.
Main outcomes and measures: Characteristics among participants randomized to either appendectomy or antibiotics were compared with those of participants who selected their own treatment.
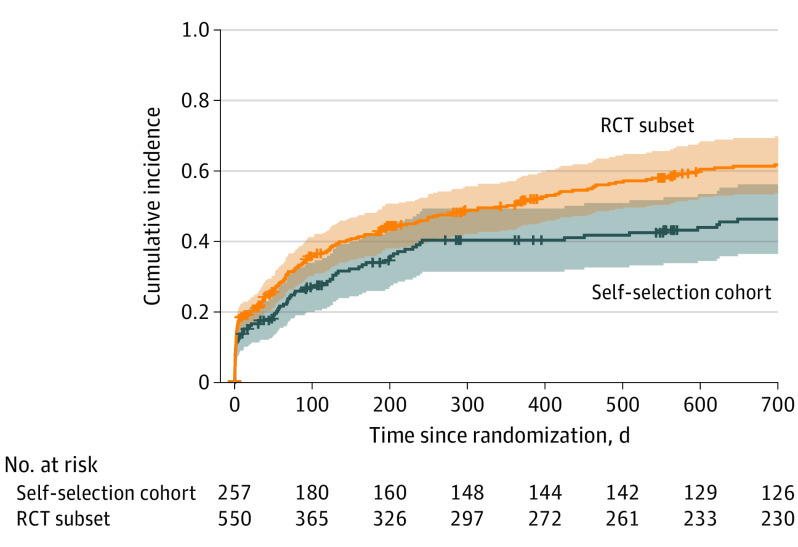
Results: Clinical characteristics were similar across the self-selection cohort (510 patients; mean age, 35.8 years [95% CI, 34.5-37.1]; 218 female [43%; 95% CI, 39%-47%]) and the randomized group (1094 patients; mean age, 38.2 years [95% CI, 37.4-39.0]; 386 female [35%; 95% CI, 33%-38%]). Compared with the randomized group, those in the self-selection cohort were less often Spanish speaking (n = 99 [19%; 95% CI, 16%-23%] vs n = 336 [31%; 95% CI, 28%-34%]), reported more formal education (some college or more, n = 355 [72%; 95% CI, 68%-76%] vs n = 674 [63%; 95% CI, 60%-65%]), and more often had commercial insurance (n = 259 [53%; 95% CI, 48%-57%] vs n = 486 [45%; 95% CI, 42%-48%]). Most outcomes were similar between the self-selection and randomized cohorts. The number of patients undergoing appendectomy by 30 days was 38 (15.3%; 95% CI, 10.7%-19.7%) among those selecting antibiotics and 155 (19.2%; 95% CI, 15.9%-22.5%) in those who were randomized to antibiotics (difference, 3.9%; 95% CI, -1.7% to 9.5%). Differences in the rate of appendectomy were primarily observed in the non-appendicolith subgroup.
Conclusions and relevance: This secondary analysis of the CODA RCT found substantially similar outcomes across the randomized and self-selection cohorts, suggesting that the randomized trial results are generalizable to the community at large.
Trial registration: ClinicalTrials.gov Identifier: NCT02800785.
Conflict of interest statement
Figures
Comment in
-
RCT Evidence Supports Incorporating Nonoperative Management Option for Uncomplicated Acute Appendicitis-How to Implement This in Clinical Practice?JAMA Surg. 2022 Jul 1;157(7):607-608. doi: 10.1001/jamasurg.2022.1555. JAMA Surg. 2022. PMID: 35612876 Clinical Trial. No abstract available.
References
-
- Turhan AN, Kapan S, Kütükçü E, Yiğitbaş H, Hatipoğlu S, Aygün E. Comparison of operative and non operative management of acute appendicitis. Ulus Travma Acil Cerrahi Derg. 2009;15(5):459-462. - PubMed
