

Agreement and Correlation Between Different Topical Corticosteroid Potency Classification Systems
- PMID: 35612864
- PMCID: PMC9134043
- DOI: 10.1001/jamadermatol.2022.1706
Agreement and Correlation Between Different Topical Corticosteroid Potency Classification Systems
Abstract
Importance: Topical corticosteroids (TCSs) are available in multiple potencies that alter their effectiveness and safety. Pharmacoepidemiologic studies on TCSs are hampered by the absence of a universal potency classification system, limiting comparisons across studies, robust exposure classification, and clinical interpretation.
Objective: To classify TCSs into 3 commonly used potency classification systems and evaluate the agreement and correlation between the 3 systems.
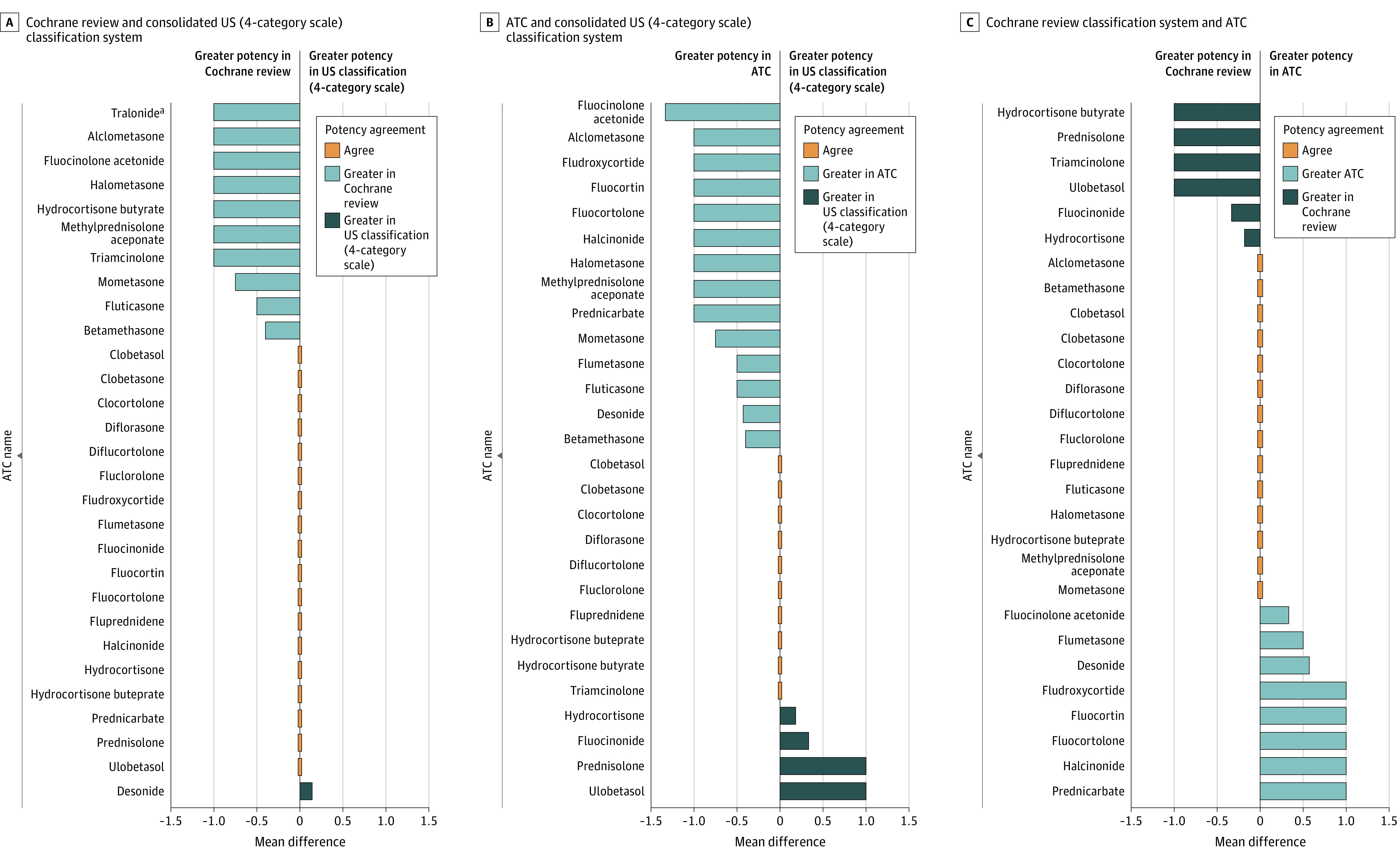
Design, setting, and participants: In this classification study, a comprehensive list of TCS formulations was compiled using sources identified in the literature, the Ontario Drug Benefit Formulary, a recent Cochrane review on the use of TCSs in people with eczema, and the Anatomical Therapeutic Classification (ATC) of the World Health Organization from August 11, 2021, to January 6, 2022. Topical corticosteroid potency classifications were assigned and compared using the 7-category US classification system, a 4-category classification from a recent Cochrane review largely based on the UK formulary, and the 4-category ATC classification. To facilitate comparisons across systems, the 7-category US system was consolidated into 4 categories.
Main outcomes and measures: Cohen weighted κ (κw) and Spearman rank correlation coefficients (r) were computed to examine agreement and correlation between the classification systems.
Results: A total of 232 unique TCS formulations (ATC, n = 231; US classification, n = 232; Cochrane review, n = 89) were included. Overall, there was low-to-moderate agreement but strong correlation between the classification systems. The US classification had weak agreement with the ATC system (κw, 0.53; 95% CI, 0.45-0.60) and moderate agreement with the Cochrane review classification (κw, 0.60; 95% CI, 0.48-0.73); there was weak agreement between the ATC and Cochrane review classifications (κw, 0.58; 95% CI, 0.46-0.71). The US classification strongly correlated with the ATC system (r, 0.77; 95% CI, 0.71-0.82) and Cochrane review classification (r, 0.74; 95% CI, 0.62-0.82). There was also a strong correlation between the Cochrane review and ATC classifications (r, 0.71; 95% CI, 0.58-0.80).
Conclusions and relevance: This classification study used multiple resources to classify 232 TCS formulations into 3 potency classifications. Because these systems are often incongruent, they may yield different results in pharmacoepidemiologic studies; investigators need to be transparent in their classification approach and consider alternative potency definitions in sensitivity analyses.
Conflict of interest statement
Figures
Comment in
-
The Power of Topical Steroids.JAMA Dermatol. 2022 Jul 1;158(7):727-729. doi: 10.1001/jamadermatol.2022.0816. JAMA Dermatol. 2022. PMID: 35612867 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
