

Combined nerve and vascular ultrasound in thoracic outlet syndrome: A sensitive method in identifying the site of neurovascular compression
- PMID: 35613111
- PMCID: PMC9132285
- DOI: 10.1371/journal.pone.0268842
Combined nerve and vascular ultrasound in thoracic outlet syndrome: A sensitive method in identifying the site of neurovascular compression
Abstract
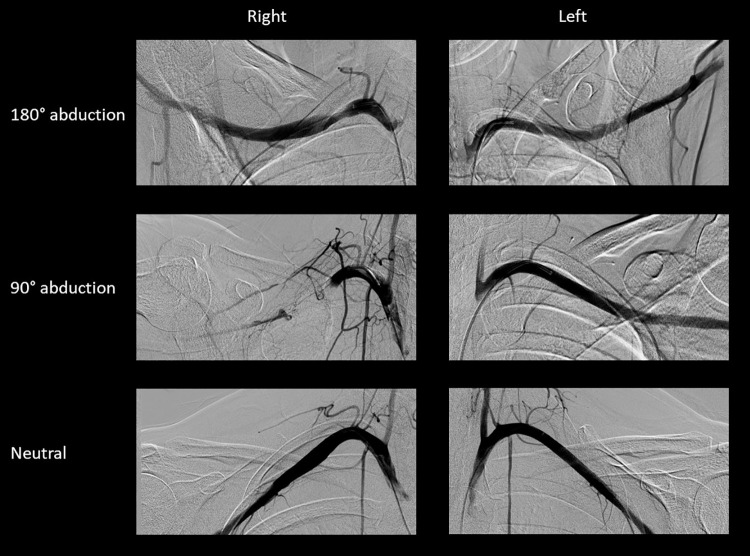
We investigated the diagnostic utility of combined nerve and vascular ultrasound in thoracic outlet syndrome (TOS) in a retrospective cohort study on two sites, involving 167 consecutive patients with the clinical symptoms suggestive of neurogenic and/or vascular TOS, and an age- and sex-matched control group. All patients and control subjects underwent nerve ultrasound of the supraclavicular brachial plexus to look for fibromuscular anomalies / compression of the brachial plexus in the scalenic region, and vascular ultrasound of the infraclavicular subclavian artery with the arm in neutral and abducted position, serving as an indicator for costoclavicular compression of the neurovascular bundle. Based on clinical symptoms, neurogenic TOS (81%) was the most frequent type of TOS, followed by combined neurogenic and arterial TOS (8%). The frequency of abnormal nerve and/or vascular ultrasound findings differed significantly from the control group (P<0.00001). The pooled sensitivity was 48% for nerve ultrasound, 85% for vascular ultrasound, and 94% when combined. Among the findings, the fibromuscular 'wedge-sickle sign', indicating compression of the lower trunk in the scalenic region by a congenital fibromuscular anomaly (e.g. Roos ligaments), showed the highest specificity (100%). A bony 'wedge-sickle sign' was also delineated, where lower trunk compression is caused by the neck of the 1st rib. As implied by the higher sensitivity of vascular ultrasound, the most common site of compression was the costoclavicular space, but multilevel compression was also frequently observed. In summary, combined nerve and vascular ultrasound is a sensitive and reliable method to support the diagnosis of TOS. It can also identify the site(s) of compression, with obvious therapeutic consequences.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






References
-
- Peete RM, Heriksen MD, Anderson TP. Thoracic outlet syndrome: evaluation of a therapeutic exercise program. Mayo Clin Proc 1956; 31:281–287. - PubMed
-
- Thompson RW in Illig KA, Thompson RW, Freischlag JA, Donahue DM, Jordan SE, Edgelow PI (Editors). Thoracic outlet syndrome. Springer-Verlag; London, 2013. pp.144, 552.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
