

Estimates of Japanese Encephalitis mortality and morbidity: A systematic review and modeling analysis
- PMID: 35613183
- PMCID: PMC9173604
- DOI: 10.1371/journal.pntd.0010361
Estimates of Japanese Encephalitis mortality and morbidity: A systematic review and modeling analysis
Abstract
Background: Japanese Encephalitis (JE) is known for its high case fatality ratio (CFR) and long-term neurological sequelae. Over the years, efforts in JE treatment and control might change the JE fatality risk. However, previous estimates were from 10 years ago, using data from cases in the 10 years before this. Estimating JE disease severity is challenging because data come from countries with different JE surveillance systems, diagnostic methods, and study designs. Without precise and timely JE disease severity estimates, there is continued uncertainty about the JE disease burden and the effect of JE vaccination.
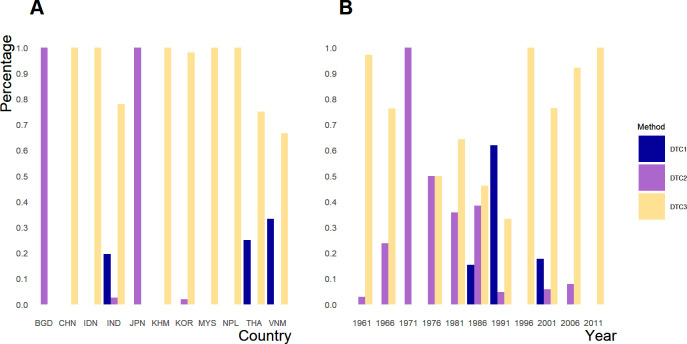
Methodology: We performed a systematic review to collate age-stratified JE fatality and morbidity data. We used a stepwise model selection with BIC as the selection criteria to identify JE CFR drivers. We used stacked regression, to predict country-specific JE CFR from 1961 to 2030. JE morbidity estimates were grouped from similar study designs to estimate the proportion of JE survivors with long-term neurological sequelae.
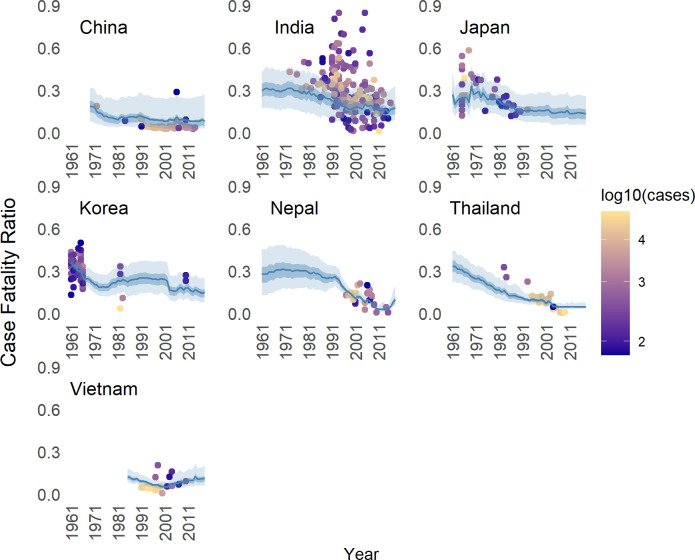
Principal findings: We included 82 and 50 peer-reviewed journal articles published as of March 06 2021 for JE fatality and morbidity with 22 articles in both analyses. Results suggested overall JE CFR estimates of 26% (95% CI 22, 30) in 1961-1979, 20% (95% CI 17, 24) in 1980-1999, 14% (95% CI 11, 17) in 2000-2018, and 14% (95% CI 11, 17) in 2019-2030. Holding other variables constant, we found that JE fatality risk decreased over time (OR: 0.965; 95% CI: 0.947-0.983). Younger JE cases had a slightly higher JE fatality risk (OR: 1.012; 95% CI: 1.003-1.021). The odds of JE fatality in countries with JE vaccination is 0.802 (90% CI: 0.653-0.994; 95% CI: 0.62-1.033) times lower than the odds in countries without JE vaccination. Ten percentage increase in the percentage of rural population to the total population was associated with 15.35% (95% CI: 7.71, 22.57) decrease in JE fatality odds. Ten percentage increase in population growth rate is associated with 3.71% (90% CI: 0.23, 7.18; 95% CI: -0.4, 8.15) increase in JE fatality odds. Adjusting for the effect of year, rural population percent, age of JE cases, and population growth rate, we estimated that there was a higher odds of JE fatality in India compared to China. (OR: 5.46, 95% CI: 3.61-8.31). Using the prediction model we found that, in 2000-2018, Brunei, Pakistan, and Timor-Leste were predicted to have the highest JE CFR of 20%. Bangladesh, Guam, Pakistan, Philippines, and Vietnam had projected JE CFR over 20% for after 2018, whereas the projected JE CFRs were below 10% in China, Indonesia, Cambodia, Myanmar, Malaysia, and Thailand. For disability, we estimated that 36% (min-max 0-85) JE patients recovered fully at hospital discharge. One year after hospital discharge, 46% (min-max 0%-97%) JE survivors were estimated to live normally but 49% (min-max 3% - 86%)till had neurological sequelae.
Conclusion: JE CFR estimates were lower than 20% after 2000. Our study provides an updated estimation of CFR and proportion of JE cases with long-term neurological sequelae that could help to refine cost-benefit assessment for JE control and elimination programs.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
-
- Hsu YH. Japanese encephalitis. Tzu Chi Med J. 2008;20(2):154.
-
- Campbell GL, Hills SL, Fischer M, Jacobson JA, Hoke CH, Hombach JM, Marfin AA, Solomon T, Tsai TF, Tsu VD, Ginsburg AS. Systematic reviews 766 Estimated global incidence of Japanese encephalitis: a systematic review. Bull World Heal Organ. 2011;89:766–74. doi: 10.2471/BLT.10.085233 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
