

Percutaneous Coronary Intervention vs. Coronary Artery Bypass Grafting for Treating In-Stent Restenosis in Unprotected-Left Main: LM-DRAGON-Registry
- PMID: 35615559
- PMCID: PMC9125786
- DOI: 10.3389/fcvm.2022.849971
Percutaneous Coronary Intervention vs. Coronary Artery Bypass Grafting for Treating In-Stent Restenosis in Unprotected-Left Main: LM-DRAGON-Registry
Abstract
Background: Data regarding management of patients with unprotected left main coronary artery in-stent restenosis (LM-ISR) are scarce.
Objectives: This study investigated the safety and effectiveness of percutaneous coronary intervention (PCI) vs. coronary artery bypass grafting (CABG) for the treatment of unprotected LM-ISR.
Methods: Consecutive patients who underwent PCI or CABG for unprotected LM-ISR were enrolled. The primary endpoint was a composite of major adverse cardiac and cerebrovascular events (MACCE), defined as cardiac death, myocardial infarction (MI), target vessel revascularization (TVR), and stroke.
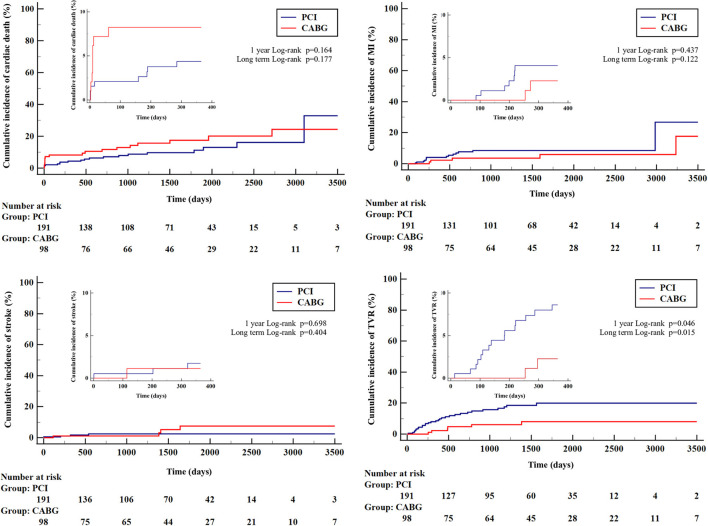
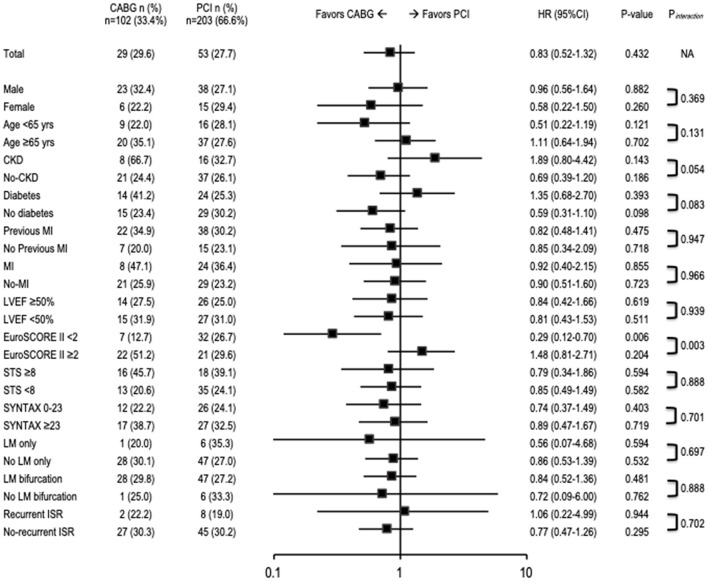
Results: A total of 305 patients were enrolled, of which 203(66.6%) underwent PCI and 102(33.4%) underwent CABG. At 30-day follow-up, a lower risk of cardiac death was observed in the PCI group, compared with the CABG-treated group (2.1% vs. 7.1%, HR 3.48, 95%CI 1.01-11.8, p = 0.04). At a median of 3.5 years [interquartile range (IQR) 1.3-5.5] follow-up, MACCE occurred in 27.7% vs. 29.6% (HR 0.82, 95%CI 0.52-1.32, p = 0.43) in PCI- and CABG-treated patients, respectively. There were no significant differences between PCI and CABG in cardiac death (9.9% vs. 18.4%; HR 1.56, 95%CI 0.81-3.00, p = 0.18), MI (7.9% vs. 5.1%, HR 0.44, 95%CI 0.15-1.27, p = 0.13), or stroke (2.1% vs. 4.1%, HR 1.79, 95%CI 0.45-7.16, p = 0.41). TVR was more frequently needed in the PCI group (15.2% vs. 6.1%, HR 0.35, 95%CI 0.15-0.85, p = 0.02).
Conclusions: This analysis of patients with LM-ISR revealed a lower incidence of cardiac death in PCI compared with CABG in short-term follow-up. During the long-term follow-up, no differences in MACCE were observed, but patients treated with CABG less often required TVR.
Visual overview: A visual overview is available for this article.
Registration: https://www.clinicaltrials.gov; Unique identifier: NCT04968977.
Keywords: coronary artery bypass graft (CABG); in-stent restenosis (ISR); left main; percutaneous coronary intervention (complex PCI); stents (Coronary).
Copyright © 2022 Wańha, Bil, Kołodziejczak, Kowalówka, Kowalewski, Hudziak, Gocoł, Januszek, Figatowski, Milewski, Tomasiewicz, Kübler, Hrymniak, Desperak, Kuźma, Milewski, Góra, Łoś, Kulczycki, Włodarczak, Skorupski, Grygier, Lesiak, D'Ascenzo, Andres, Kleczynski, Litwinowicz, Borin, Smolka, Reczuch, Gruchała, Gil, Jaguszewski, Bartuś, Suwalski, Dobrzycki, Dudek, Bartuś, Ga̧sior, Ochała, Lansky, Deja, Legutko, Kedhi and Wojakowski.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Makikallio T, Holm NR, Lindsay M, Spence MS, Erglis A, Menown IB, et al. . Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis (NOBLE): a prospective, randomised, open-label, non-inferiority trial. Lancet. (2016) 388:2743–52. 10.1016/S0140-6736(16)32052-9 - DOI - PubMed
-
- Sheiban I, Sillano D, Biondi-Zoccai G, Chieffo A, Colombo A, Vecchio S, et al. . Incidence and management of restenosis after treatment of unprotected left main disease with drug-eluting stents 70 restenotic cases from a cohort of 718 patients: FAILS (Failure in Left Main Study). J Am Coll Cardiol. (2009) 54:1131–6. 10.1016/j.jacc.2009.06.018 - DOI - PubMed
-
- Lee JY, Park DW, Kim YH, Yun SC, Kim WJ, Kang SJ, et al. . Incidence, predictors, treatment, and long-term prognosis of patients with restenosis after drug-eluting stent implantation for unprotected left main coronary artery disease. J Am Coll Cardiol. (2011) 57:1349–58. 10.1016/j.jacc.2010.10.041 - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous