

A Multifaceted Evaluation of a COVID-19 Contact Tracing Program in King County, Washington
- PMID: 35616571
- PMCID: PMC9119327
- DOI: 10.1097/PHH.0000000000001541
A Multifaceted Evaluation of a COVID-19 Contact Tracing Program in King County, Washington
Abstract
Context: Despite the massive scale of COVID-19 case investigation and contact tracing (CI/CT) programs operating worldwide, the evidence supporting the intervention's public health impact is limited.
Objective: To evaluate the Public Health-Seattle & King County (PHSKC) CI/CT program, including its reach, timeliness, effect on isolation and quarantine (I&Q) adherence, and potential to mitigate pandemic-related hardships.
Design: This program evaluation used descriptive statistics to analyze surveillance records, case and contact interviews, referral records, and survey data provided by a sample of cases who had recently ended isolation.
Setting: The PHSKC is one of the largest governmental local health departments in the United States. It serves more than 2.2 million people who reside in Seattle and 38 other municipalities.
Participants: King County residents who were diagnosed with COVID-19 between July 2020 and June 2021.
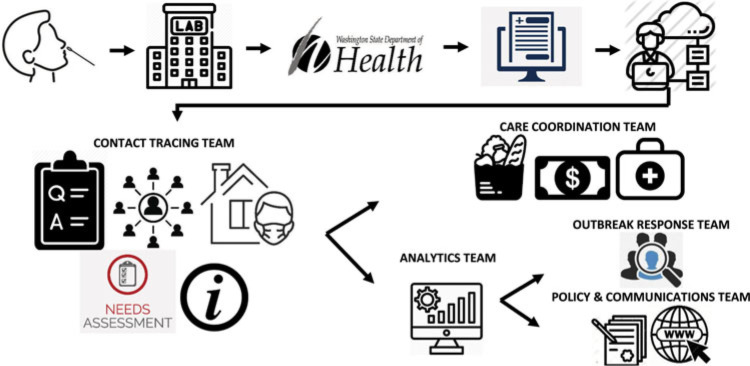
Intervention: The PHSKC integrated COVID-19 CI/CT with prevention education and service provision.
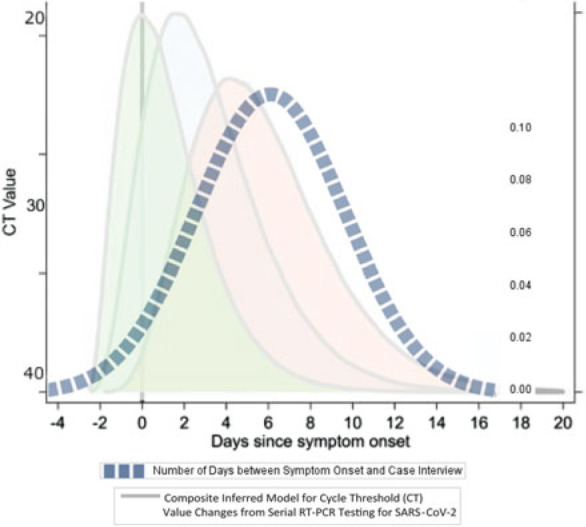
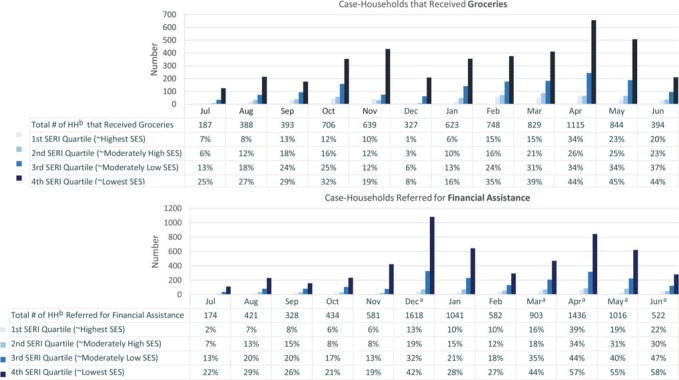
Results: The PHSKC CI/CT team interviewed 42 900 cases (82% of cases eligible for CI/CT), a mean of 6.1 days after symptom onset and 3.4 days after SARS-CoV-2 testing. Cases disclosed the names and addresses of 10 817 unique worksites (mean = 0.8/interview) and 11 432 other recently visited locations (mean = 0.5/interview) and provided contact information for 62 987 household members (mean = 2.7/interview) and 14 398 nonhousehold contacts (mean = 0.3/interview). The CI/CT team helped arrange COVID-19 testing for 5650 contacts, facilitated grocery delivery for 7253 households, and referred 9127 households for financial assistance. End of I&Q Survey participants (n = 304, 54% of sampled) reported self-notifying an average of 4 nonhousehold contacts and 69% agreed that the information and referrals provided by the CI/CT team helped them stay in isolation.
Conclusions: In the 12-month evaluation period, CI/CT reached 42 611 households and identified thousands of exposure venues. The timing of CI/CT relative to infectiousness and difficulty eliciting nonhousehold contacts may have attenuated the intervention's effect. Through promotion of I&Q guidance and services, CI/CT can help mitigate pandemic-related hardships.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
COVID-19 Case Investigation and Contact Tracing in the US, 2020.JAMA Netw Open. 2021 Jun 1;4(6):e2115850. doi: 10.1001/jamanetworkopen.2021.15850. JAMA Netw Open. 2021. PMID: 34081135 Free PMC article.
-
Design, Implementation, and Outcomes of a Volunteer-Staffed Case Investigation and Contact Tracing Initiative at an Urban Academic Medical Center.JAMA Netw Open. 2022 Sep 1;5(9):e2232110. doi: 10.1001/jamanetworkopen.2022.32110. JAMA Netw Open. 2022. PMID: 36149656 Free PMC article.
-
COVID-19 Contact Tracing Outcomes in Washington State, August and October 2020.Front Public Health. 2021 Nov 26;9:782296. doi: 10.3389/fpubh.2021.782296. eCollection 2021. Front Public Health. 2021. PMID: 34900921 Free PMC article.
-
Interplay of demographics, geography and COVID-19 pandemic responses in the Puget Sound region: The Vashon, Washington Medical Reserve Corps experience.PLoS One. 2023 Aug 16;18(8):e0274345. doi: 10.1371/journal.pone.0274345. eCollection 2023. PLoS One. 2023. PMID: 37585489 Free PMC article.
-
Building Case Investigation and Contact Tracing Programs in US State and Local Health Departments: A Conceptual Framework.Disaster Med Public Health Prep. 2023 Nov 30;17:e540. doi: 10.1017/dmp.2023.205. Disaster Med Public Health Prep. 2023. PMID: 38031272 Review.
Cited by
-
Modernizing the Objectives and Organization of Case Investigation and Contact Tracing for the 21st Century.Sex Transm Dis. 2023 Aug 1;50(8S Suppl 1):S6-S13. doi: 10.1097/OLQ.0000000000001697. Epub 2022 Aug 16. Sex Transm Dis. 2023. PMID: 35969847 Free PMC article.
-
Quantifying the impact of contact tracing interview prioritisation strategies on disease transmission: A modelling study.PLoS Comput Biol. 2025 Apr 4;21(4):e1012906. doi: 10.1371/journal.pcbi.1012906. eCollection 2025 Apr. PLoS Comput Biol. 2025. PMID: 40184558 Free PMC article.
-
Accuracy of Inferences About the Reproductive Number and Superspreading Potential of SARS-CoV-2 with Incomplete Contact Tracing Data.Res Sq [Preprint]. 2023 Dec 29:rs.3.rs-3760127. doi: 10.21203/rs.3.rs-3760127/v1. Res Sq. 2023. PMID: 38234843 Free PMC article. Preprint.
-
Measuring Success: Disease Intervention Specialists Performance Metrics and Outcome Assessments.Sex Transm Dis. 2023 Aug 1;50(8S Suppl 1):S18-S22. doi: 10.1097/OLQ.0000000000001740. Epub 2022 Nov 21. Sex Transm Dis. 2023. PMID: 36730526 Free PMC article.
-
Meeting Social Needs in a Crisis Context: Lessons Learned from Integrating the 'Take Care Initiative' into New York City's Testing and Contact Tracing Program.J Urban Health. 2024 Oct;101(5):902-912. doi: 10.1007/s11524-024-00900-9. Epub 2024 Sep 12. J Urban Health. 2024. PMID: 39266870
References
-
- Resolve to Save Lives. Press release: new contact tracing playbook provides guidance to public health officials on nationwide efforts to contain COVID-19. https://resolvetosavelives.org/about/press/new-contact-tracing-playbook. Published 2020. Accessed September 28, 2021.
-
- Centers for Disease Control and Prevention. Interim guidance on developing a COVID-19 case investigation & contact tracing plan: overview. https://www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tr.... Published 2021. Accessed September 28, 2021.
-
- Centers for Disease Control and Prevention. Scaling up staffing roles in case investigation and contact tracing. https://www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tr.... Published 2021. Accessed September 28, 2021.
-
- National Academies of Sciences E, and Medicine. Encouraging Participation and Cooperation in Contact Tracing: Lessons From Survey Research. Washington, DC: The National Academies Press; 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
