

Cancer Risk C (CR-C), a functional genomics test is a sensitive and rapid test for germline mismatch repair deficiency
- PMID: 35616648
- PMCID: PMC10072225
- DOI: 10.1016/j.gim.2022.05.003
Cancer Risk C (CR-C), a functional genomics test is a sensitive and rapid test for germline mismatch repair deficiency
Abstract
Purpose: Heritable pathogenic variants in the DNA mismatch repair (MMR) pathway cause Lynch syndrome, a condition that significantly increases risk of colorectal and other cancers. At least half of individuals tested using gene panel sequencing have a variant of uncertain significance or no variant identified leading to no diagnosis. To fill this diagnostic gap, we developed Cancer Risk C (CR-C), a flow variant assay test.
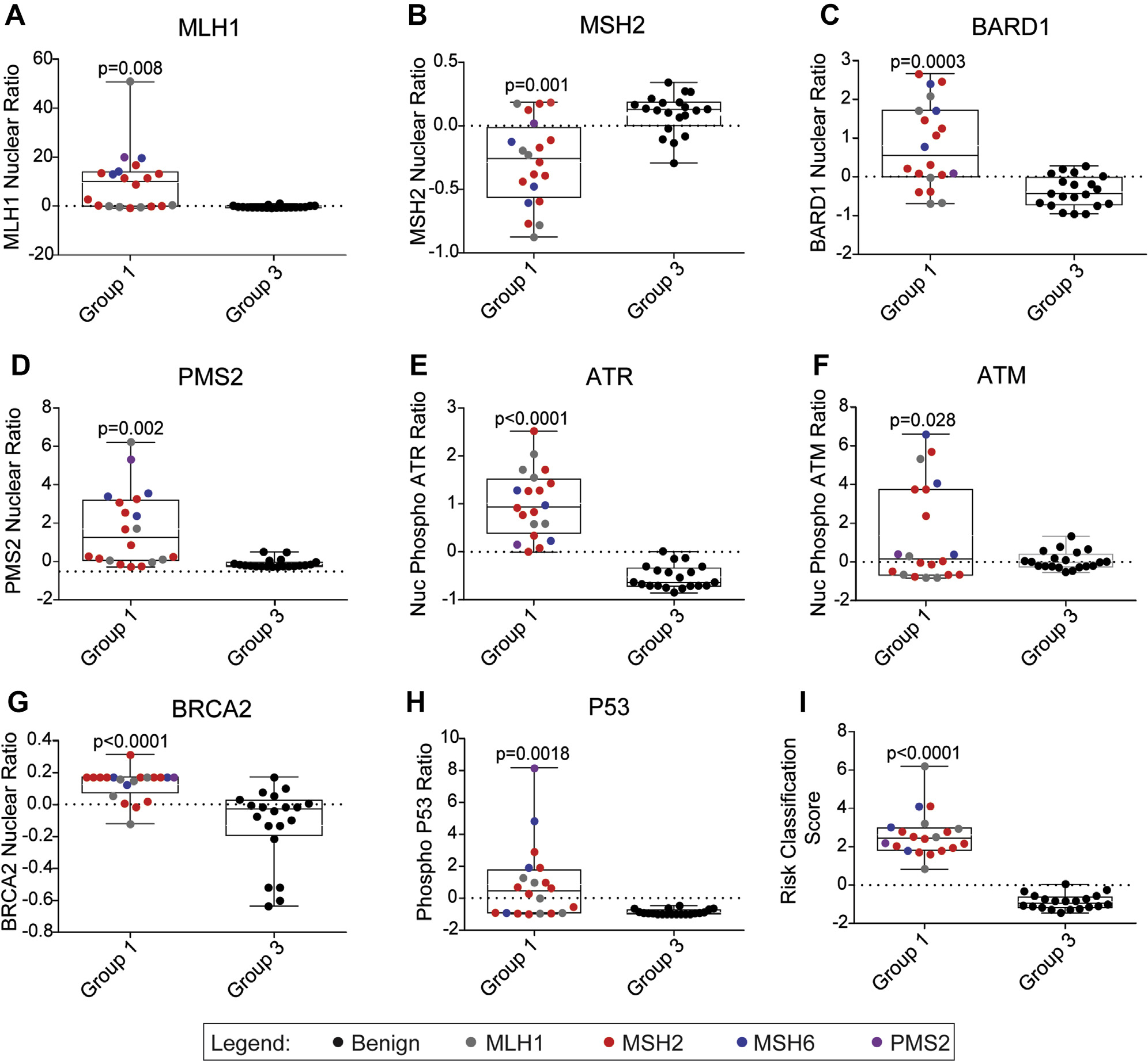
Methods: In response to treatment with an alkylating agent, individual assays of the nuclear translocation of MLH1, MSH2, BARD1, PMS2, and BRCA2 proteins and the nuclear phosphorylation of the ATM and ATR proteins distinguished pathogenic/likely pathogenic (P/LP) from benign/likely benign variants in MMR genes.
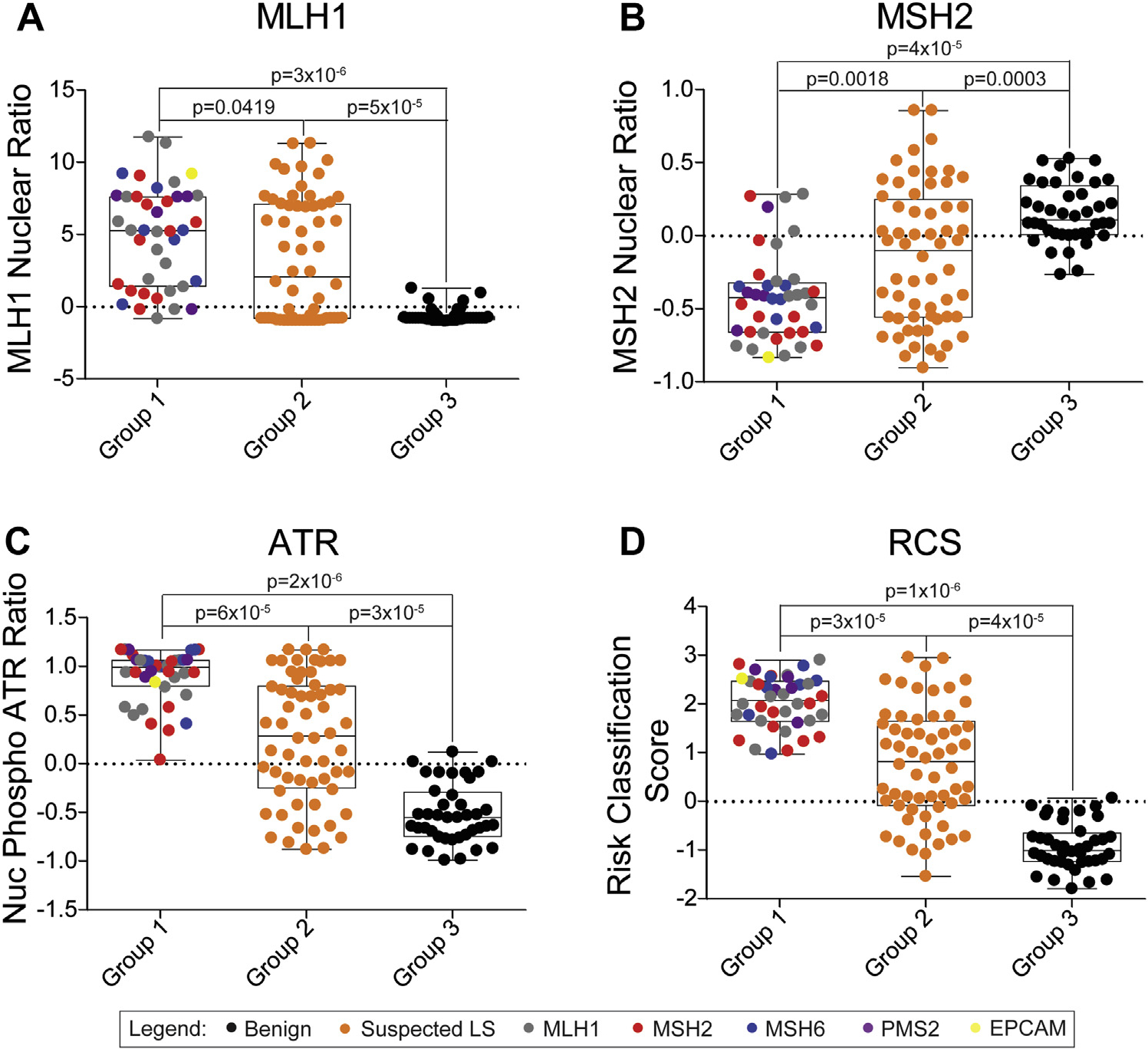
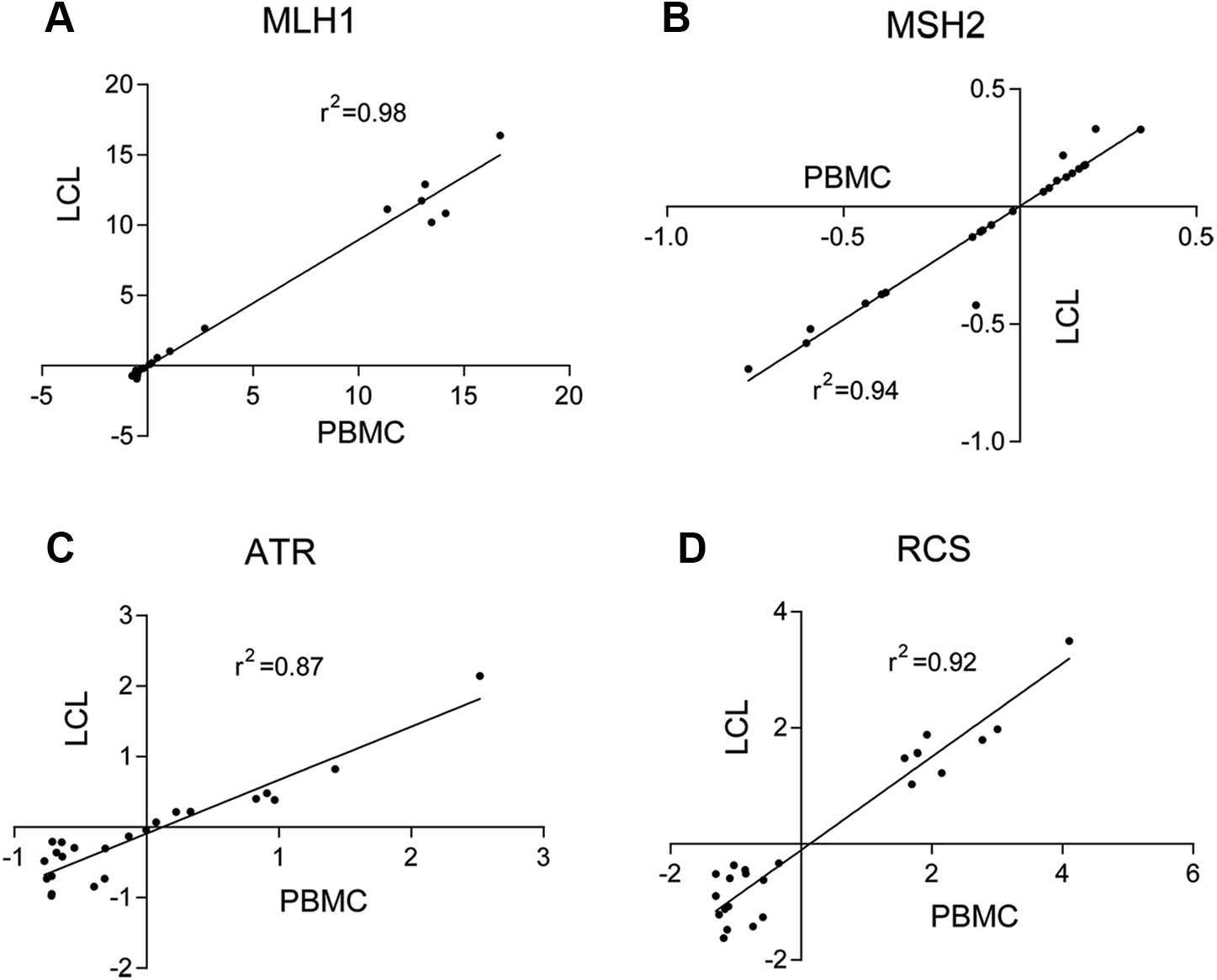
Results: A risk classification score based on MLH1, MSH2, and ATR assays was 100% sensitive and 98% specific. Causality of MMR P/LP variants was shown through gene editing and rescue. In individuals with suspected Lynch syndrome but no P/LP, CR-C identified most (73%) as having germline MMR defects. Direct comparison of CR-C on matched blood samples and lymphoblastoid cell lines yielded comparable results (r2 > 0.9).
Conclusion: For identifying germline MMR defects, CR-C provides augmentation to traditional panel sequencing through greater accuracy, shorter turnaround time (48 hours), and performance on blood with minimal sample handling.
Keywords: Colorectal cancer; Functional genomics; Genetic testing; Lynch syndrome; Variant of uncertain significance.
Copyright © 2022 American College of Medical Genetics and Genomics. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest H.O. and J.L. are members of the scientific advisory board for Morgan & Mendel Genomics Inc and own shares of the company. I.A., S.Y., A.S.T., P.N., N.M.L., R.K.P., M.A.J., D.D.B., S.G., and S.K. declare no conflicts of interest.
Figures

Similar articles
-
Advances in genetic technologies result in improved diagnosis of mismatch repair deficiency in colorectal and endometrial cancers.J Med Genet. 2022 Apr;59(4):328-334. doi: 10.1136/jmedgenet-2020-107542. Epub 2021 Jan 15. J Med Genet. 2022. PMID: 33452216 Free PMC article.
-
Germline variants screening of MLH1, MSH2, MSH6 and PMS2 genes in 64 Algerian Lynch syndrome families: The first nationwide study.Ann Hum Genet. 2022 Nov;86(6):328-352. doi: 10.1111/ahg.12482. Epub 2022 Sep 8. Ann Hum Genet. 2022. PMID: 36073783
-
Rare germline mutation and MSH2-&MSH6 + expression in a double primary carcinoma of colorectal carcinoma and endometrial carcinoma: a case report.Diagn Pathol. 2024 Jan 31;19(1):25. doi: 10.1186/s13000-024-01447-8. Diagn Pathol. 2024. PMID: 38297350 Free PMC article.
-
Muir-Torre Syndrome and founder mismatch repair gene mutations: A long gone historical genetic challenge.Gene. 2016 Sep 10;589(2):127-32. doi: 10.1016/j.gene.2015.06.078. Epub 2015 Jul 2. Gene. 2016. PMID: 26143115 Review.
-
Update on Lynch syndrome genomics.Fam Cancer. 2016 Jul;15(3):385-93. doi: 10.1007/s10689-016-9882-8. Fam Cancer. 2016. PMID: 26873718 Free PMC article. Review.
Cited by
-
Germline Variants in MLH1 and ATM Genes in a Young Patient with MSI-H in a Precancerous Colonic Lesion.Int J Mol Sci. 2023 Mar 22;24(6):5970. doi: 10.3390/ijms24065970. Int J Mol Sci. 2023. PMID: 36983044 Free PMC article.
-
Lynch syndrome, molecular mechanisms and variant classification.Br J Cancer. 2023 Mar;128(5):726-734. doi: 10.1038/s41416-022-02059-z. Epub 2022 Nov 24. Br J Cancer. 2023. PMID: 36434153 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
