

Association of Nighttime Masked Uncontrolled Hypertension With Left Ventricular Hypertrophy and Kidney Function Among Patients with Chronic Kidney Disease Not Receiving Dialysis
- PMID: 35616936
- PMCID: PMC9136624
- DOI: 10.1001/jamanetworkopen.2022.14460
Association of Nighttime Masked Uncontrolled Hypertension With Left Ventricular Hypertrophy and Kidney Function Among Patients with Chronic Kidney Disease Not Receiving Dialysis
Abstract
Importance: Nighttime hypertension is prevalent and associated with adverse outcomes in patients with chronic kidney disease (CKD), but nighttime hypertension, a subtype of masked uncontrolled hypertension (MUCH), is often undetected among patients with controlled office blood pressure. Little attention has been paid to patients with CKD and nighttime MUCH.
Objective: To investigate the prevalence of nighttime MUCH and its associations with cardiovascular and kidney outcomes in patients with CKD who were not receiving dialysis.
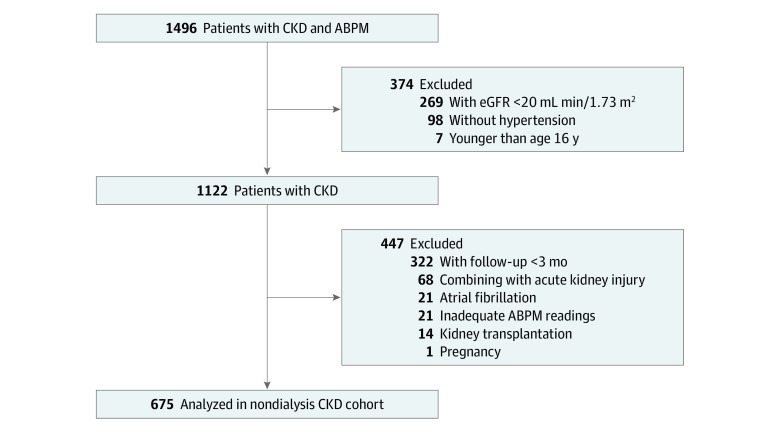
Design, setting, and participants: This retrospective cohort study included patients with nondialysis CKD and hypertension, enrolled in Shanghai, China, from July 2012 through November 2020 and followed up for a median of 39 months.
Exposures: Participants were classified as having controlled hypertension, sustained hypertension, and MUCH, which was further divided into isolated nighttime MUCH and day-night MUCH, assessed by office and ambulatory blood pressure monitoring.
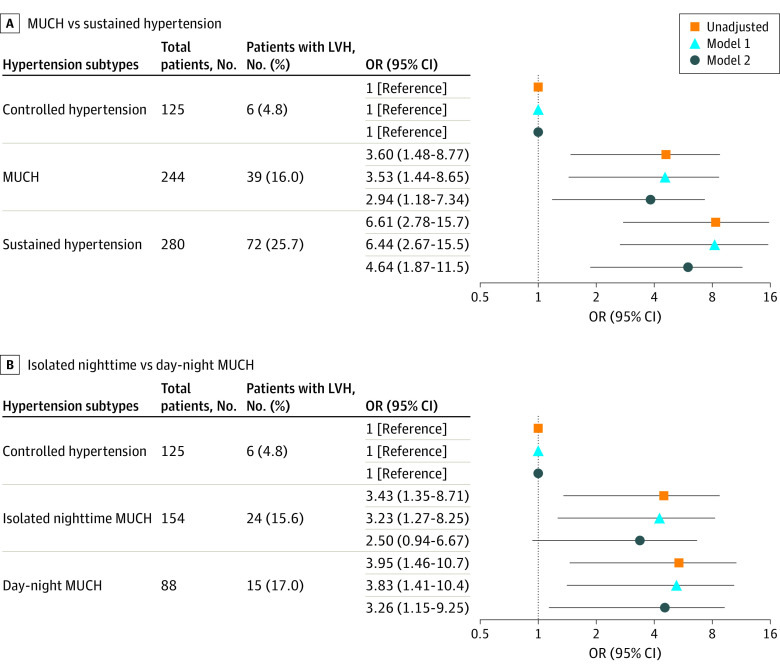
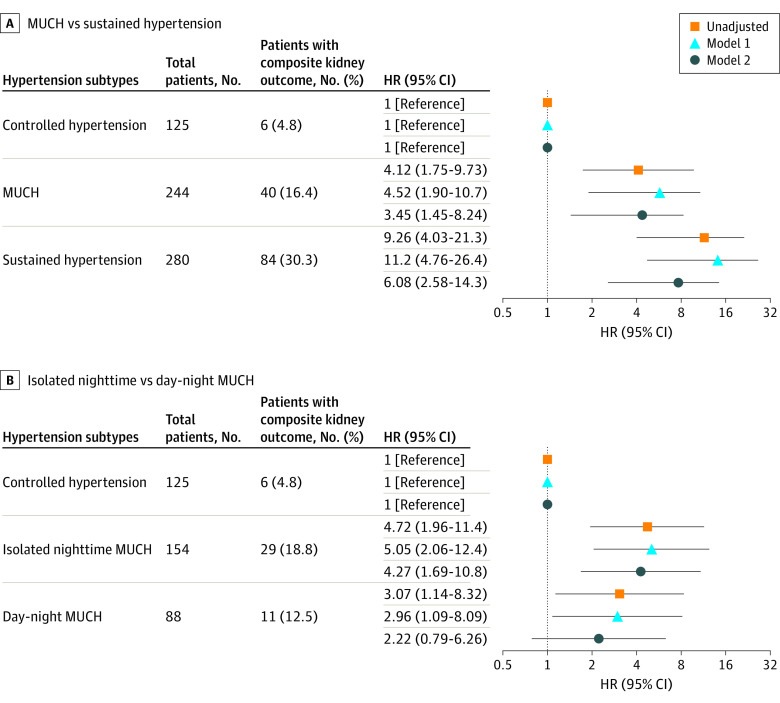
Main outcomes and measures: Left ventricular hypertrophy (LVH) was determined by echocardiography. The composite kidney outcome consisted of end-stage kidney diseases (ESKD) and a reduction of estimated glomerular filtration rate (eGFR) by 50% or more. Logistic and Cox regression assessed the associations of hypertension subtypes with LVH and kidney outcomes.
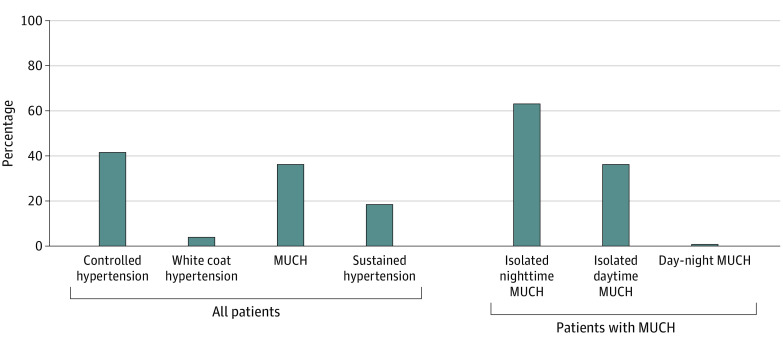
Results: The 675 patients (425 [63.0%] men; mean [SD] age, 50.8 [15.9] years; mean [SD] eGFR, 61.6 [29.4] mL/min/1.73 m2) included 125 (19.3%) with controlled hypertension, 244 (37.6%) with MUCH, and 280 (43.1%) sustained hypertension. Among patients with MUCH, 2 (0.8%) had isolated daytime MUCH, 154 (63.1%) had isolated nighttime MUCH, and 88 (36.1%) had day-night MUCH. During a median (IQR) follow-up of 39 (19-64) months, 130 composite kidney events, including 97 ESKD events, occurred. Compared with controlled hypertension, MUCH and sustained hypertension were associated with LVH (eg, MUCH: odds ratio [OR], 2.94; 95% CI, 1.18-7.34; P = .02) and the composite kidney outcome (eg, MUCH: hazard ratio [HR], 4.12; 95% CI, 1.75-9.73; P = .001) after adjustment for age, sex, proteinuria, eGFR, and other baseline risk factors. Multivariate-adjusted associations were also significant between day-night MUCH and LVH (OR, 3.26; 95% CI, 1.15-9.25) and between isolated nighttime MUCH and the composite kidney outcome (HR, 4.27; 95% CI, 1.69-10.77).
Conclusions and relevance: In this cohort study, nighttime MUCH was common and associated with LVH and poor kidney outcomes among patients with hypertension and nondialysis CKD. These findings suggest that ambulatory blood pressure monitoring was inadequately used in patients with CKD and hypertension, calling for more widespread use, even in patients with controlled office hypertension.
Conflict of interest statement
Figures
Comment in
-
Nighttime Hypertension in Chronic Kidney Disease-Are We in the Dark Without Ambulatory Blood Pressure Monitoring?JAMA Netw Open. 2022 May 2;5(5):e2214469. doi: 10.1001/jamanetworkopen.2022.14469. JAMA Netw Open. 2022. PMID: 35616944 No abstract available.
References
-
- Buckalew VM Jr, Berg RL, Wang SR, Porush JG, Rauch S, Schulman G; Modification of Diet in Renal Disease Study Group . Prevalence of hypertension in 1,795 subjects with chronic renal disease: the modification of diet in renal disease study baseline cohort. Am J Kidney Dis. 1996;28(6):811-821. doi: 10.1016/S0272-6386(96)90380-7 - DOI - PubMed
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):e127-e248. doi: 10.1016/j.jacc.2017.11.006 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
