

Thromboembolic Risk in Patients With Pneumonia and New-Onset Atrial Fibrillation Not Receiving Anticoagulation Therapy
- PMID: 35616941
- PMCID: PMC9136621
- DOI: 10.1001/jamanetworkopen.2022.13945
Thromboembolic Risk in Patients With Pneumonia and New-Onset Atrial Fibrillation Not Receiving Anticoagulation Therapy
Abstract
Importance: New-onset atrial fibrillation (AF) is commonly reported in patients with severe infections. However, the absolute risk of thromboembolic events without anticoagulation remains unknown.
Objective: To investigate the thromboembolic risks associated with AF in patients with pneumonia, assess the risk of recurrent AF, and examine the association of initiation of anticoagulation therapy with new-onset AF.
Design, setting, and participants: This population-based cohort study used linked Danish nationwide registries. Participants included patients hospitalized with incident community-acquired pneumonia in Denmark from 1998 to 2018. Statistical analysis was performed from August 15, 2021, to March 12, 2022.
Exposures: New-onset AF.
Main outcomes and measures: Thromboembolic events, recurrent AF, and all-cause death. Estimated risks were calculated for thromboembolism without anticoagulation therapy, new hospital or outpatient clinic contact with AF, initiation of anticoagulation therapy, and all-cause death at 1 and 3 years of follow-up. Death was treated as a competing risk, and inverse probability of censoring weights was used to account for patient censoring if they initiated anticoagulation therapy conditioned on AF.
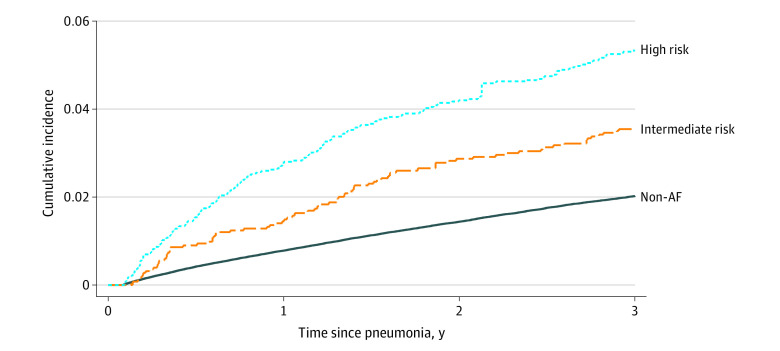
Results: Among 274 196 patients hospitalized for community-acquired pneumonia, 6553 patients (mean age [SD], 79.1 [11.0] years; 3405 women [52.0%]) developed new-onset AF. The 1-year risk of thromboembolism was 0.8% (95% CI, 0.8%-0.8%) in patients without AF vs 2.1% (95% CI, 1.8%-2.5%) in patients with new-onset AF without anticoagulation; this risk was 1.4% (95% CI, 1.0%-2.0%) among patients with AF with intermediate stroke risk and 2.8% (95% CI, 2.3%-3.4%) in patients with AF with high stroke risk. Three-year risks were 3.5% (95% CI, 2.8%-4.3%) among patients with intermediate stroke risk and 5.3% (95% CI, 4.4%-6.5%) among patients with high stroke risk. Among patients with new-onset AF, 32.9% (95% CI, 31.8%-34.1%) had a new hospital contact with AF, and 14.0% (95% CI, 13.2%-14.9%) initiated anticoagulation therapy during the 3 years after incident AF diagnosis. At 3 years, the all-cause mortality rate was 25.7% (95% CI, 25.6%-25.9%) in patients with pneumonia without AF vs 49.8% (95% CI, 48.6%-51.1%) in patients with new-onset AF.
Conclusions and relevance: This cohort study found that new-onset AF after community-acquired pneumonia was associated with an increased risk of thromboembolism, which may warrant anticoagulation therapy. Approximately one-third of patients had a new hospital or outpatient clinic contact for AF during the 3-year follow-up, suggesting that AF triggered by acute infections is not a transient, self-terminating condition that reverses with resolution of the infection.
Conflict of interest statement
Figures
References
-
- Hall MJ, DeFrances CJ, Williams SN, Golosinskiy A, Schwartzman A. National Hospital Discharge Survey: 2007 summary. Natl Health Stat Report. 2010;(29):1-20, 24. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
