

Takotsubo cardiomyopathy in patients suffering from acute non-traumatic subarachnoid hemorrhage-A single center follow-up study
- PMID: 35617162
- PMCID: PMC9135260
- DOI: 10.1371/journal.pone.0268525
Takotsubo cardiomyopathy in patients suffering from acute non-traumatic subarachnoid hemorrhage-A single center follow-up study
Abstract
Background: Takotsubo cardiomyopathy (TTC) is an important complication of subarachnoid hemorrhage (SAH), that may delay surgical or endovascular treatment and may influence patient outcome. This prospective follow-up study intended to collect data on the prevalence, severity, influencing factors and long-term outcome of TTC in patients suffering from non-traumatic SAH.
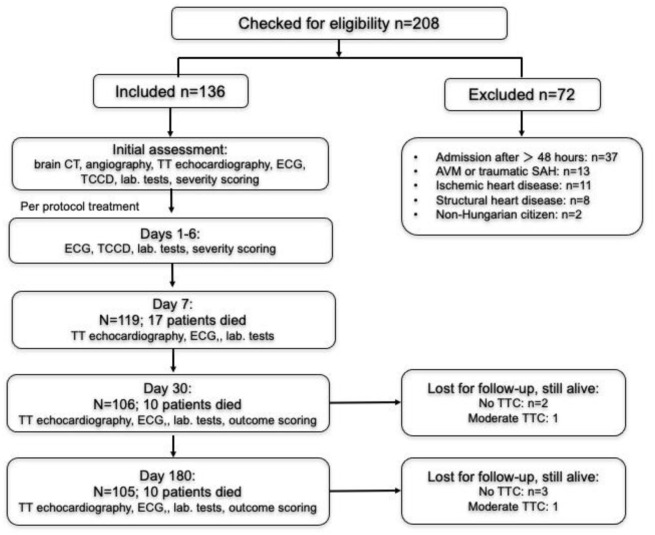
Methods: Consecutive patients admitted with the diagnosis of non-traumatic SAH were included. Intitial assessment consisted of cranial CT, Hunt-Hess, Fisher and WFNS scoring, 12-lead ECG, transthoracic echocardiography (TTE), transcranial duplex sonography and collecting laboratory parameters (CK, CK-MB, cardiac troponin T, NT-proBNP and urine metanephrine and normetanephrine). Diagnosis of TTC was based on modified Mayo criteria. TTC patients were dichotomized to mild and severe forms. Follow-up of TTE, Glasgow Outcome Scale assessment, Barthel's and Karnofsky scoring occurred on days 30 and 180.
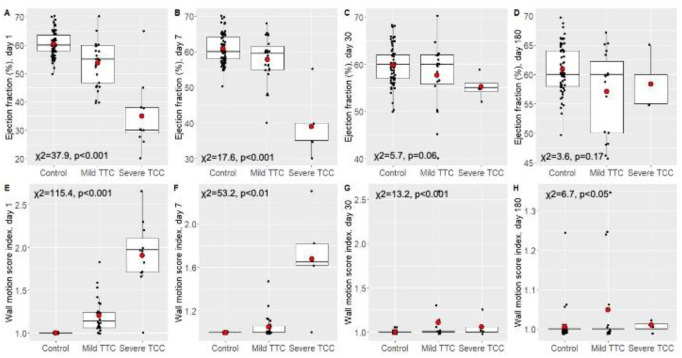
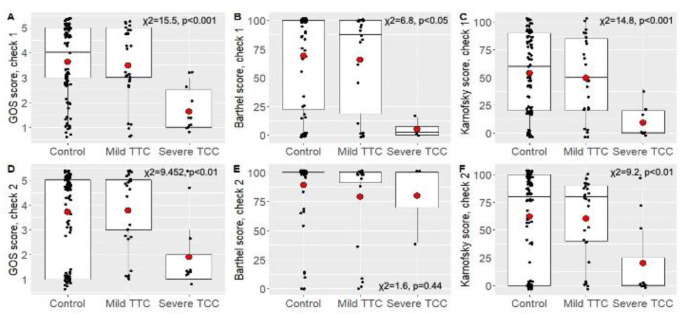
Results: One hundred thirty six patients were included. The incidence of TTC in the entire cohort was 28.7%; of them, 20.6% and 8.1% were mild and severe, respectively. TTC was more frequent in females (30/39; 77%) than in males (9/39; 23%) and was more severe. The occurrence of TTC was related to mFisher scores and WFNS scores. Although the severity of TTC was related to mFisher score, Hunt-Hess score, WFNS score and GCS, multivariate analysis showed the strongest relationship with mFisher scores. Ejection fraction differences between groups were present on day 30, but disappeared by day 180, whereas wall motion score index was still higher in the severe TTC group at day 180. By the end of the follow-up period (180 days), 70 (74.5%) patients survived in the non-TTC, 22 (81.5%) in the mild TTC and 3 (27%) in the severe TTC group (n = 11) (p = 0.002). At day 180, GOS, Barthel, and Karnofsky outcome scores were higher in patients in the control (non-TTC) and the mild TTC groups than in the severe TTC group.
Conclusions: Takotsubo cardiomyopathy is a frequent finding in patients with SAH, and severe TTC may be present in 8% of SAH cases. The severity of TTC may be an independent predictor of mortality and outcome at 6 months after disease onset. Therefore, a regular follow-up of ECG and TTE abnormalities is warranted in patients with subrachnoid hemorrhage for early detection of TTC.
Trial registration: The study was registered at the Clinical Trials Register under the registration number of NCT02659878 (date of registration: January 21, 2016).
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Differences between Takotsubo cardiomyopathy and reverse Takotsubo cardiomyopathy associated with subarachnoid hemorrhage.Int J Cardiol Heart Vasc. 2016 May 11;11:99-103. doi: 10.1016/j.ijcha.2016.05.010. eCollection 2016 Jun. Int J Cardiol Heart Vasc. 2016. PMID: 28616533 Free PMC article.
-
Outcome after Hunt and Hess Grade V subarachnoid hemorrhage: a comparison of pre-coiling era (1980-1995) versus post-ISAT era (2005-2014).J Neurosurg. 2018 Jan;128(1):100-110. doi: 10.3171/2016.8.JNS161075. Epub 2017 Feb 24. J Neurosurg. 2018. PMID: 28298025
-
Radiodensity of intraventricular hemorrhage associated with aneurysmal subarachnoid hemorrhage may be a negative predictor of outcome.J Neurosurg. 2018 Apr;128(4):1032-1036. doi: 10.3171/2016.11.JNS152839. Epub 2017 May 5. J Neurosurg. 2018. PMID: 28474990
-
Electrocardiographic and Seasonal Patterns Allow Accurate Differentiation of Tako-Tsubo Cardiomyopathy from Acute Anterior Myocardial Infarction: Results of a Multicenter Study and Systematic Overview of Available Studies.Biomolecules. 2019 Jan 30;9(2):51. doi: 10.3390/biom9020051. Biomolecules. 2019. PMID: 30704132 Free PMC article.
-
Subarachnoidal hemorrhage related cardiomyopathy: an overview of Tako-Tsubo cardiomyopathy and related cardiac syndromes.Expert Rev Cardiovasc Ther. 2022 Sep;20(9):733-745. doi: 10.1080/14779072.2022.2125871. Epub 2022 Sep 21. Expert Rev Cardiovasc Ther. 2022. PMID: 36124824 Review.
Cited by
-
Diagnosis and Management of Takotsubo Syndrome in Acute Aneurysmal Subarachnoid Hemorrhage: A Comprehensive Review.Rev Cardiovasc Med. 2023 Jun 19;24(6):177. doi: 10.31083/j.rcm2406177. eCollection 2023 Jun. Rev Cardiovasc Med. 2023. PMID: 39077518 Free PMC article. Review.
-
An Unusual Etiology: Subarachnoid Hemorrhage Resulting in Transient Apical Ballooning Syndrome.J Med Cases. 2022 Nov;13(11):541-544. doi: 10.14740/jmc4018. Epub 2022 Nov 27. J Med Cases. 2022. PMID: 36506760 Free PMC article.
-
Correlation of Inflammatory Parameters with the Development of Cerebral Vasospasm, Takotsubo Cardiomyopathy, and Functional Outcome after Spontaneous Subarachnoid Hemorrhage.J Clin Med. 2024 Mar 28;13(7):1955. doi: 10.3390/jcm13071955. J Clin Med. 2024. PMID: 38610720 Free PMC article.
-
Acute Multidisciplinary Management of Aneurysmal Subarachnoid Hemorrhage (aSAH).Balkan Med J. 2023 Mar 8;40(2):74-81. doi: 10.4274/balkanmedj.galenos.2023.2023-1-100. Balkan Med J. 2023. PMID: 36883719 Free PMC article. Review.
-
An Extensive Review on Imaging Diagnosis Methods in Takotsubo Syndrome.Rev Cardiovasc Med. 2023 Oct 20;24(10):300. doi: 10.31083/j.rcm2410300. eCollection 2023 Oct. Rev Cardiovasc Med. 2023. PMID: 39077560 Free PMC article. Review.
References
-
- Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases [in Japanese]. J Cardiol 1991;21:203–214. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
