

A recombinant monoclonal-based Taenia antigen assay that reflects disease activity in extra-parenchymal neurocysticercosis
- PMID: 35617367
- PMCID: PMC9176767
- DOI: 10.1371/journal.pntd.0010442
A recombinant monoclonal-based Taenia antigen assay that reflects disease activity in extra-parenchymal neurocysticercosis
Abstract
Background: Antigen tests for diagnosis and disease monitoring in some types of neurocysticercosis (NCC) are useful but access to testing has been limited by availability of proprietary reagents and/or kits.
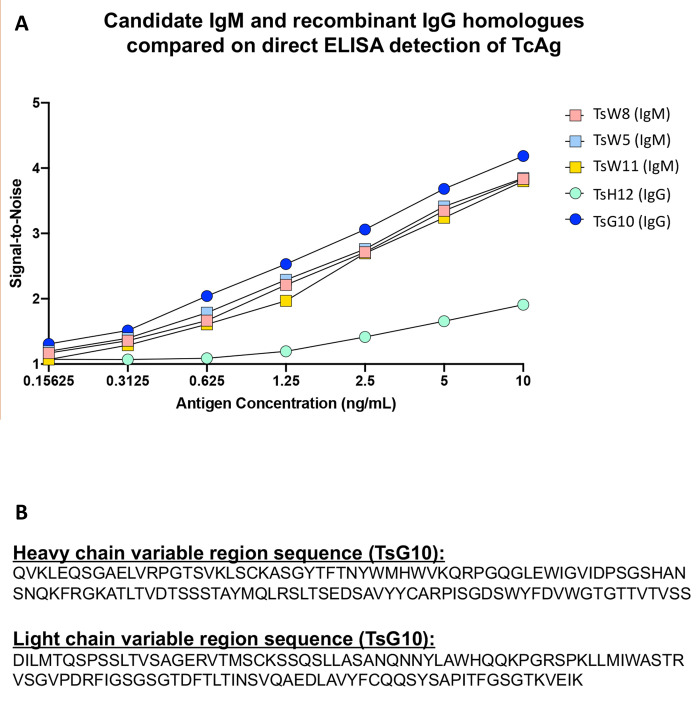
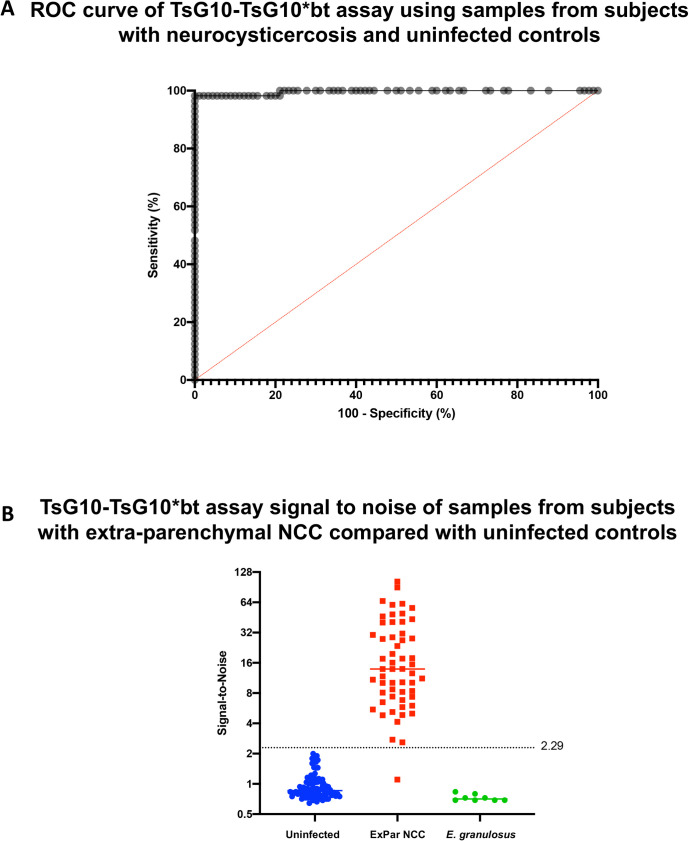
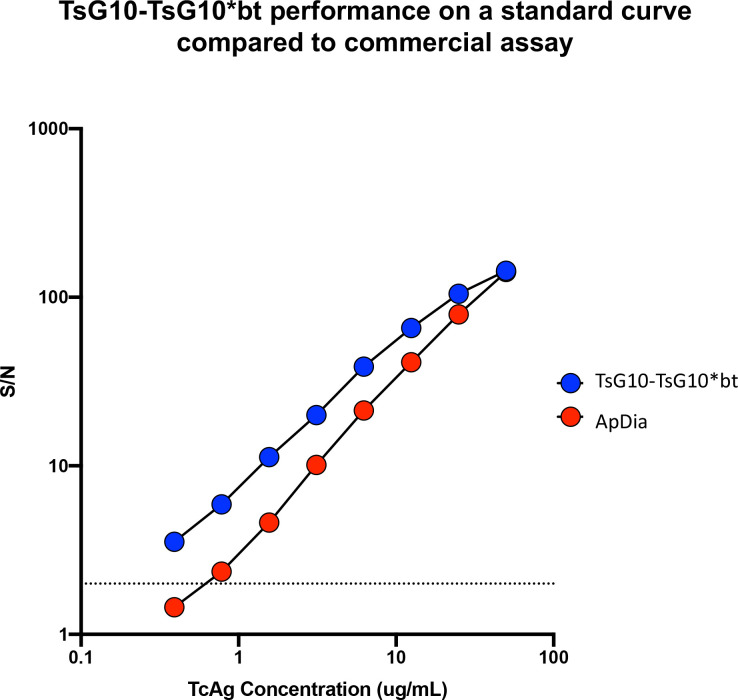
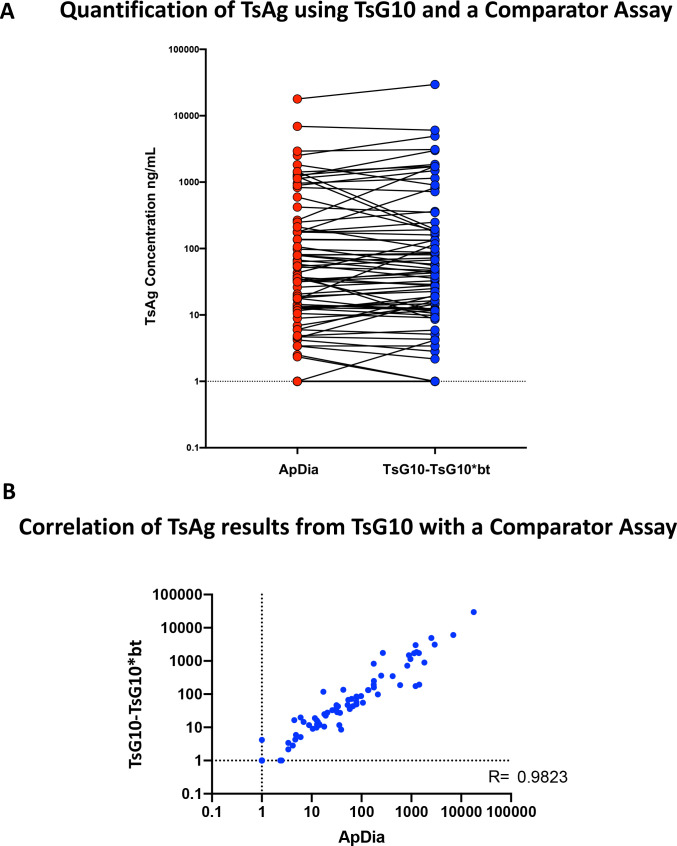
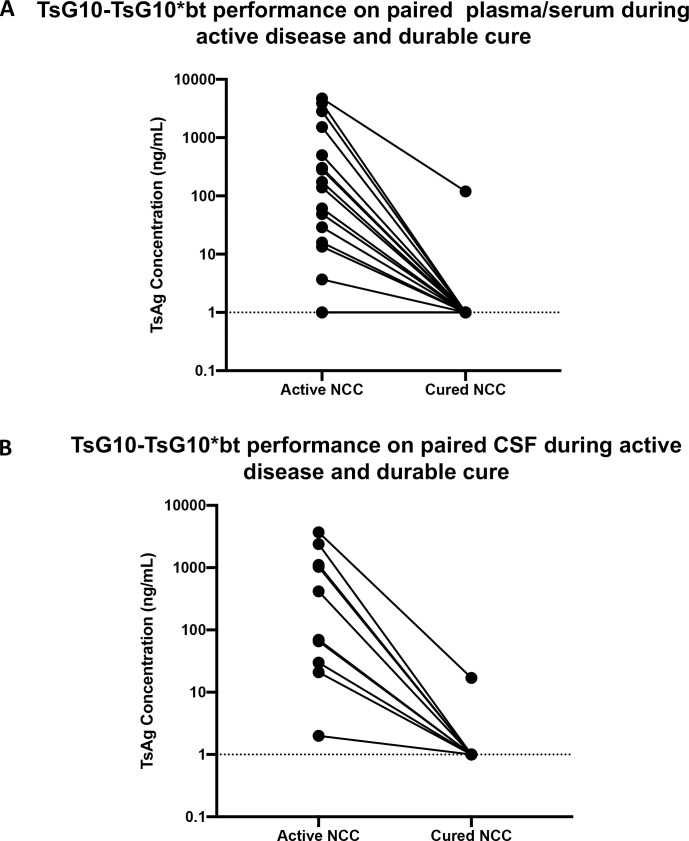
Methods/principal findings: Three previously identified IgM-secreting hybridomas whose IgM products demonstrated specificity to Taenia solium underwent variable heavy and light chain sequencing and isotype conversion to mouse IgG. Screening of these recombinantly expressed IgG anti-Ts hybridomas, identified one (TsG10) with the highest affinity to crude Taenia antigen. TsG10 was then used as a capture antibody in a sandwich antigen detection immunoassay in combination with either a high titer polyclonal anti-Ts antibody or with biotinylated TsG10 (termed TsG10*bt). Using serum, plasma, and CSF samples from patients with active NCC and those from NCC-uninfected patients, ROC curve analyses demonstrated that the TsG10-TsG10-*bt assay achieved a 98% sensitivity and 100% specificity in detecting samples known to be antigen positive and outperformed the polyclonal based assay (sensitivity of 93% with 100% specificity). By comparing levels of Ts antigen (Ag) in paired CSF (n = 10) or plasma/serum (n = 19) samples from well-characterized patients with extra-parenchymal NCC early in infection and at the time of definitive cure, all but 2 (1 from CSF and 1 from plasma) became undetectable. There was a high degree of correlation (r = 0.98) between the Ag levels detected by this new assay and levels found by a commercial assay. Pilot studies indicate that this antigen can be detected in the urine of patients with active NCC.
Conclusions/significance: A newly developed recombinant monoclonal antibody-based Ts Ag detection immunoassay is extremely sensitive in the detection of extra-parenchymal NCC and can be used to monitor the success of treatment in the CSF, serum/plasma and urine. The ability to produce recombinant TsG10 at scale should enable use of this antigen detection immunoassay wherever NCC is endemic.
Clinical trial registration: ClinicalTrials.gov Identifiers: NCT00001205 - & NCT00001645.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- O’Connell EM, Harrison S, Dahlstrom E, Nash T, Nutman TB. A novel, highly sensitive qPCR assay for the diagnosis of subarachnoid and ventricular neurocysticercosis and for assessing response to treatment. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2019. Epub 2019/06/25. doi: 10.1093/cid/ciz541 - DOI - PMC - PubMed
-
- Fleury A, Hernandez M, Avila M, Cardenas G, Bobes RJ, Huerta M, et al. Detection of HP10 antigen in serum for diagnosis and follow-up of subarachnoidal and intraventricular human neurocysticercosis. J Neurol Neurosurg Psychiatry. 2007;78(9):970–4. Epub 2007/03/06. doi: 10.1136/jnnp.2006.107243 ; PubMed Central PMCID: PMC2117888. - DOI - PMC - PubMed
-
- Rodriguez S, Dorny P, Tsang VC, Pretell EJ, Brandt J, Lescano AG, et al. Detection of Taenia solium antigens and anti-T. solium antibodies in paired serum and cerebrospinal fluid samples from patients with intraparenchymal or extraparenchymal neurocysticercosis. The Journal of infectious diseases. 2009;199(9):1345–52. Epub 2009/04/11. doi: 10.1086/597757 ; PubMed Central PMCID: PMC4059603. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
