

Non-specific effects of BCG and DTP vaccination on infant mortality: An analysis of birth cohorts in Ghana and Tanzania
- PMID: 35618557
- PMCID: PMC9194613
- DOI: 10.1016/j.vaccine.2022.04.082
Non-specific effects of BCG and DTP vaccination on infant mortality: An analysis of birth cohorts in Ghana and Tanzania
Abstract
Background: Vaccines may induce non-specific effects on survival and health outcomes, in addition to protection against targeted pathogens or disease. Observational evidence suggests that infant Baccillus Calmette-Guérin (BCG) vaccination may provide non-specific survival benefits, while diphtheria-tetanus-pertussis (DTP) vaccination may increase the risk of mortality. Non-specific vaccine effects have been hypothesized to modify the effect of neonatal vitamin A supplementation (NVAS) on mortality.
Methods: 22,955 newborns in Ghana and 31,999 newborns in Tanzania were enrolled in two parallel, randomized, double-blind, placebo-controlled trials of neonatal vitamin A supplementation from 2010 to 2014 and followed until 1-year of age. Cox proportional hazard models were used to estimate associations of BCG and DTP vaccination with infant survival.
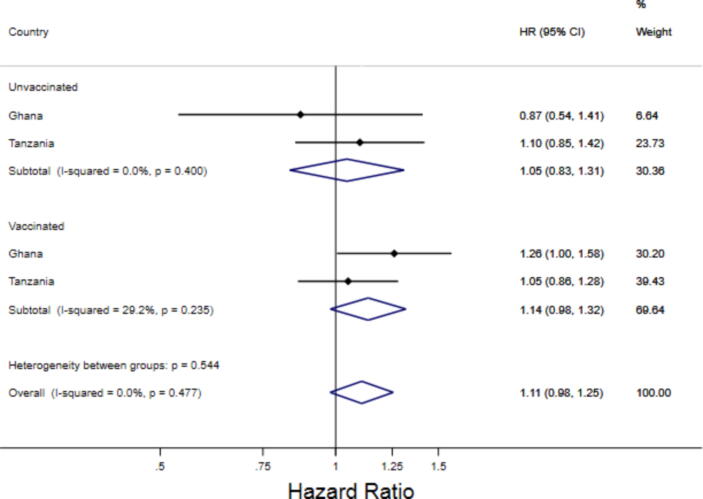
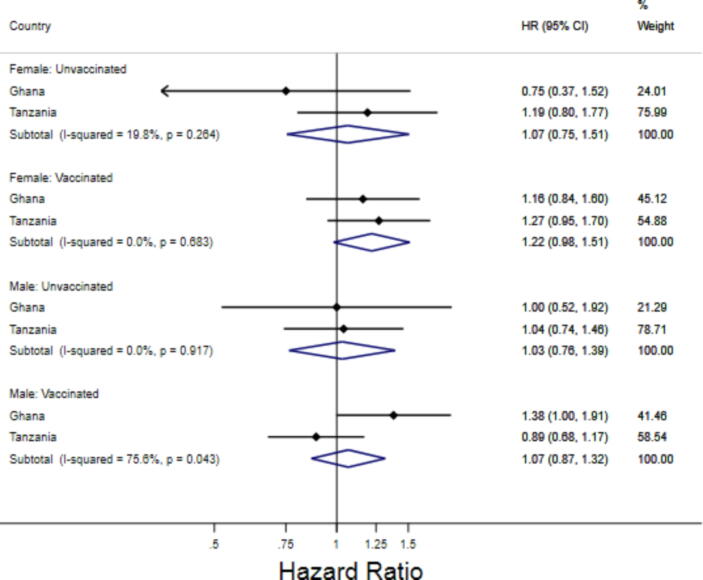
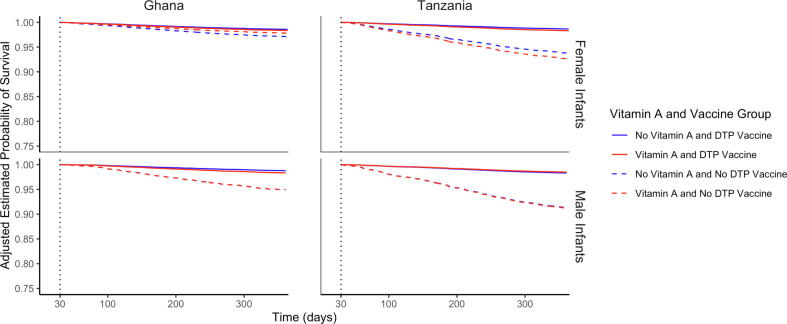
Results: BCG vaccination was associated with a decreased risk of infant mortality after controlling for confounders in both countries (Ghana adjusted hazard ratio (aHR): 0.51, 95% CI: 0.38-0.68; Tanzania aHR: 0.08, 95% CI: 0.07-0.10). Receiving a DTP vaccination was associated with a decreased risk of death (Ghana aHR: 0.39, 95% CI: 0.26-0.59; Tanzania aHR: 0.19, 95% CI: 0.16-0.22). There was no evidence of interaction between BCG or DTP vaccination status and infant sex or NVAS.
Conclusion: We demonstrated that BCG and DTP vaccination were associated with decreased risk of infant mortality in Ghana and Tanzania with no evidence of interaction between DTP or BCG vaccination, NVAS, and infant sex. Our study supports global recommendations on BCG and DTP vaccination and programmatic efforts to ensure all children have access to timely vaccination.
Clinical trials registration: Ghana (Australian New Zealand Clinical Trials Registry (ANZCTR): ACTRN12610000582055) and Tanzania (ANZCTR: ACTRN12610000636055).
Keywords: BCG Vaccine; DTP Vaccine; Infant mortality; Vitamin A.
Copyright © 2022. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Retesting the hypothesis that early Diphtheria-Tetanus-Pertussis vaccination increases female mortality: An observational study within a randomised trial.Vaccine. 2022 Mar 8;40(11):1606-1616. doi: 10.1016/j.vaccine.2021.06.008. Epub 2021 Jun 30. Vaccine. 2022. PMID: 34217570 Clinical Trial.
-
Sex-differential effects on mortality of BCG and diphtheria-tetanus-pertussis vaccines in a rural area with high vaccination coverage: observational study from Senegal.Trans R Soc Trop Med Hyg. 2016 Sep;110(9):527-533. doi: 10.1093/trstmh/trw059. Epub 2016 Oct 13. Trans R Soc Trop Med Hyg. 2016. PMID: 27738283
-
Early diphtheria-tetanus-pertussis vaccination associated with higher female mortality and no difference in male mortality in a cohort of low birthweight children: an observational study within a randomised trial.Arch Dis Child. 2012 Aug;97(8):685-91. doi: 10.1136/archdischild-2011-300646. Epub 2012 Feb 13. Arch Dis Child. 2012. PMID: 22331681 Free PMC article.
-
Combining vitamin A and vaccines: convenience or conflict?Dan Med J. 2012 Jan;59(1):B4378. Dan Med J. 2012. PMID: 22239846 Review.
-
Lessons Learned from the Testing of Neonatal Vitamin A Supplementation.Nutrients. 2019 Feb 21;11(2):449. doi: 10.3390/nu11020449. Nutrients. 2019. PMID: 30795563 Free PMC article. Review.
Cited by
-
Innovations, Challenges, and Future Prospects for Combination Vaccines Against Human Infections.Vaccines (Basel). 2025 Mar 21;13(4):335. doi: 10.3390/vaccines13040335. Vaccines (Basel). 2025. PMID: 40333234 Free PMC article. Review.
-
Training vs. Tolerance: The Yin/Yang of the Innate Immune System.Biomedicines. 2023 Mar 2;11(3):766. doi: 10.3390/biomedicines11030766. Biomedicines. 2023. PMID: 36979747 Free PMC article. Review.
-
Effects of Silirum®-Based Vaccination Programs on Map Fecal Shedding and Serological Response in Seven French Dairy Herds.Animals (Basel). 2023 May 8;13(9):1569. doi: 10.3390/ani13091569. Animals (Basel). 2023. PMID: 37174606 Free PMC article.
-
The 2024 resurgence of Bordetella pertussis in Brazil and a decade-long epidemiological overview.Front Public Health. 2025 May 27;13:1549735. doi: 10.3389/fpubh.2025.1549735. eCollection 2025. Front Public Health. 2025. PMID: 40496447 Free PMC article.
-
Protection of infant mice against pertussis, tuberculosis and influenza by co-administration of nasal pertussis vaccine candidate BPZE1 and BCG.iScience. 2025 Jun 7;28(7):112839. doi: 10.1016/j.isci.2025.112839. eCollection 2025 Jul 18. iScience. 2025. PMID: 40612502 Free PMC article.
References
-
- Lehmann D., Vail J., Firth M.J., de Klerk N.H., Alpers M.P. Benefits of routine immunizations on childhood survival in Tari, Southern Highlands Province. Papua New Guinea Int J Epidemiol. 2005;34:138–148. - PubMed
-
- Aaby P., Ravn H., Roth A., Rodrigues A., Lisse I.M., Diness B.R., et al. Early diphtheria-tetanus-pertussis vaccination associated with higher female mortality and no difference in male mortality in a cohort of low birthweight children: an observational study within a randomised trial. Arch Dis Child. 2012;97(8):685–691. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
