

Performance of plasma phosphorylated tau 181 and 217 in the community
- PMID: 35618838
- PMCID: PMC9329262
- DOI: 10.1038/s41591-022-01822-2
Performance of plasma phosphorylated tau 181 and 217 in the community
Erratum in
-
Author Correction: Performance of plasma phosphorylated tau 181 and 217 in the community.Nat Med. 2023 Nov;29(11):2954. doi: 10.1038/s41591-022-02066-w. Nat Med. 2023. PMID: 36216947 No abstract available.
Abstract
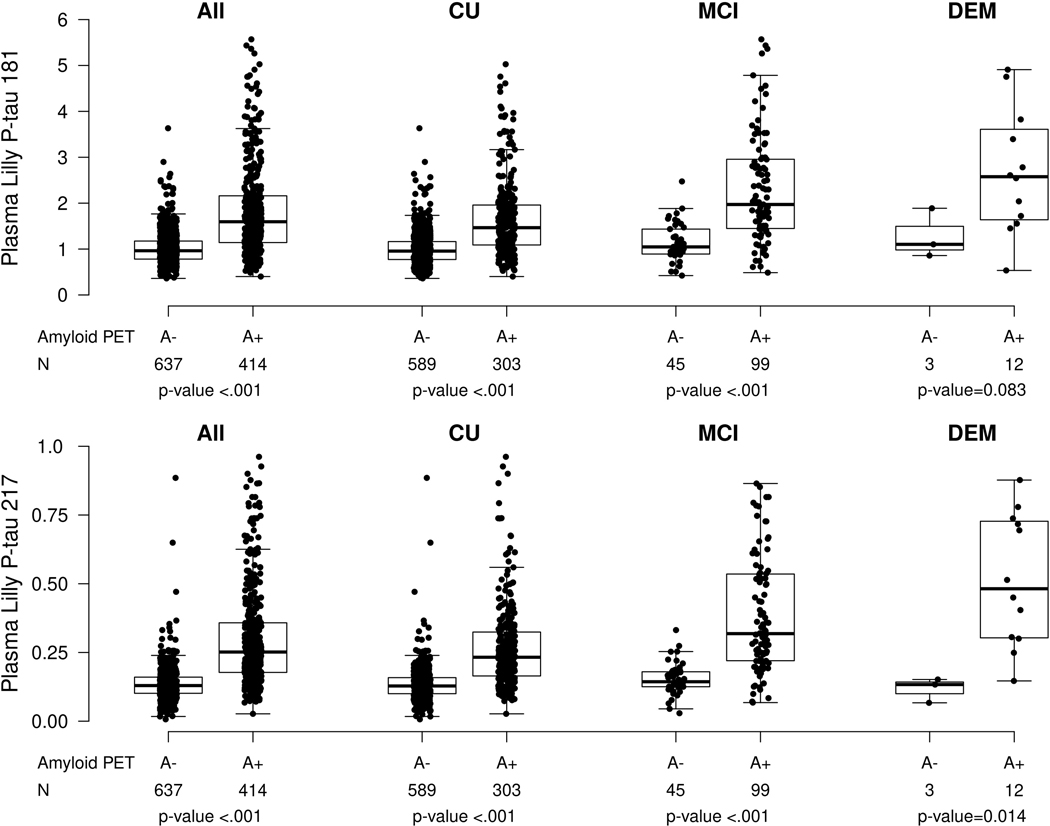
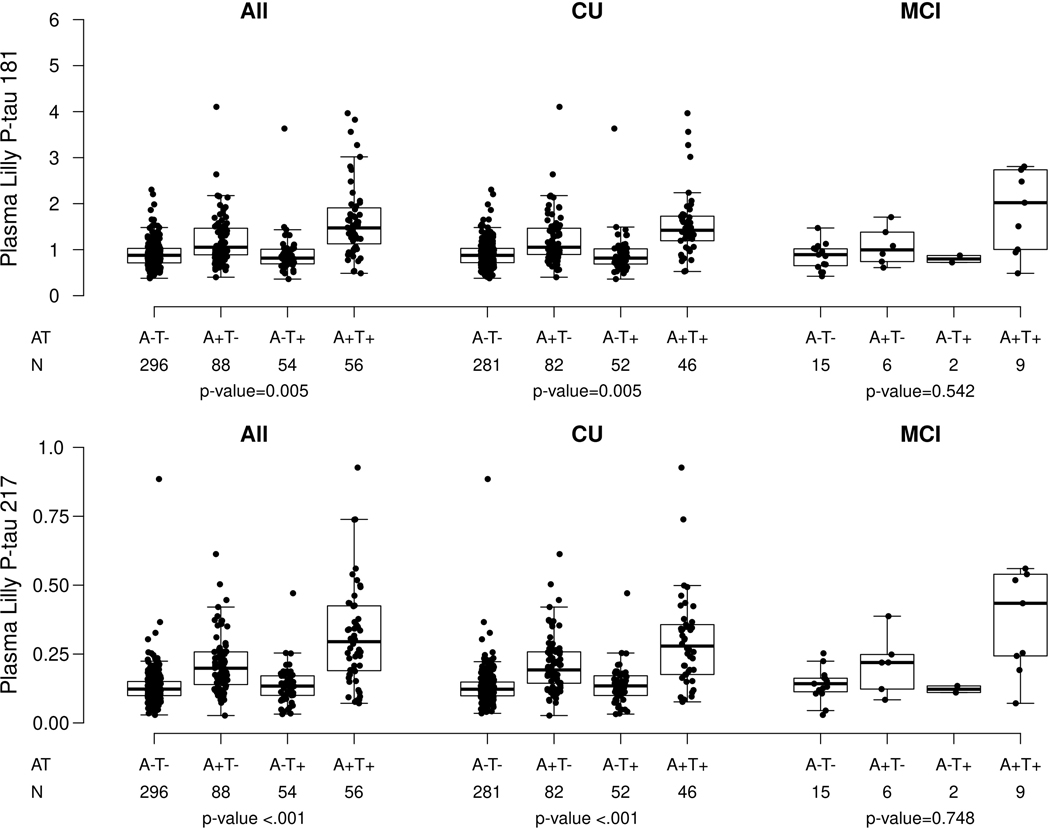
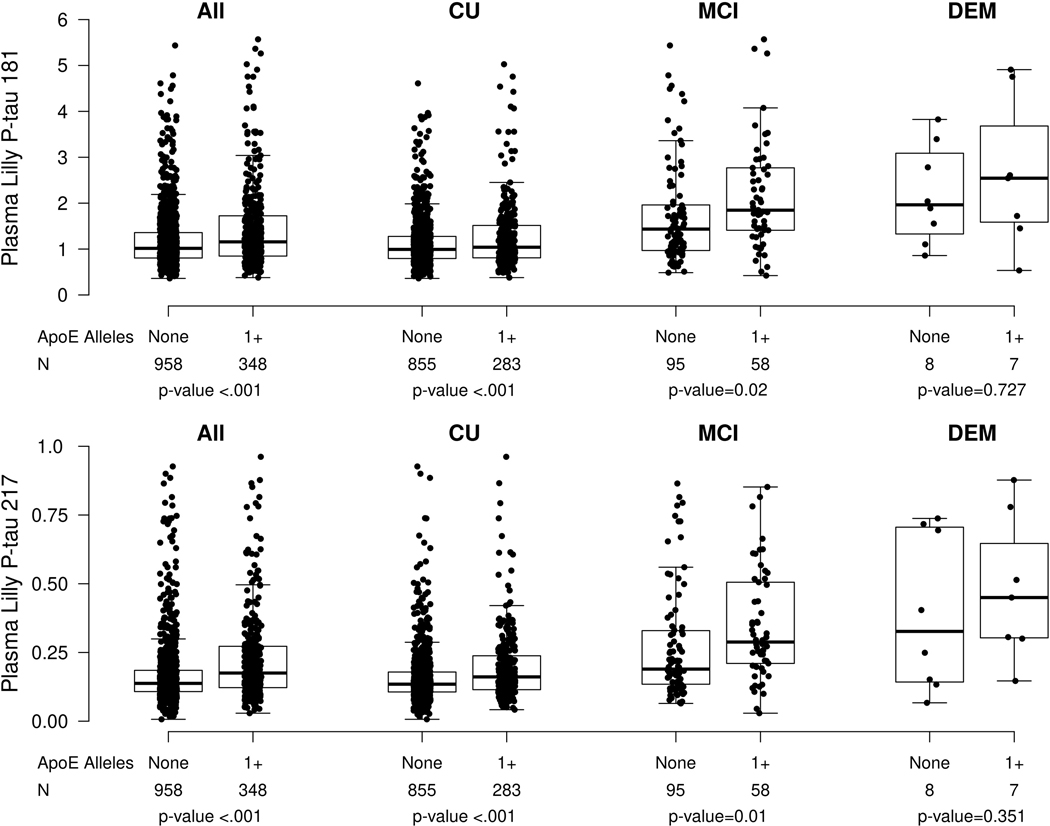
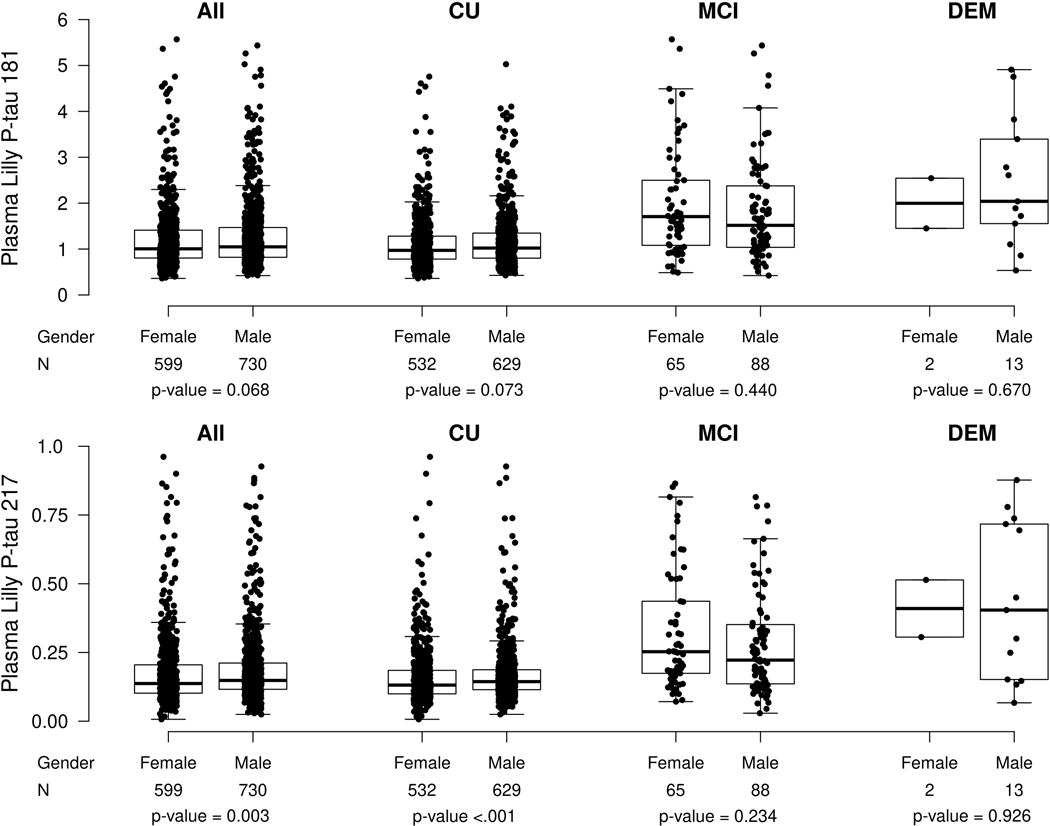
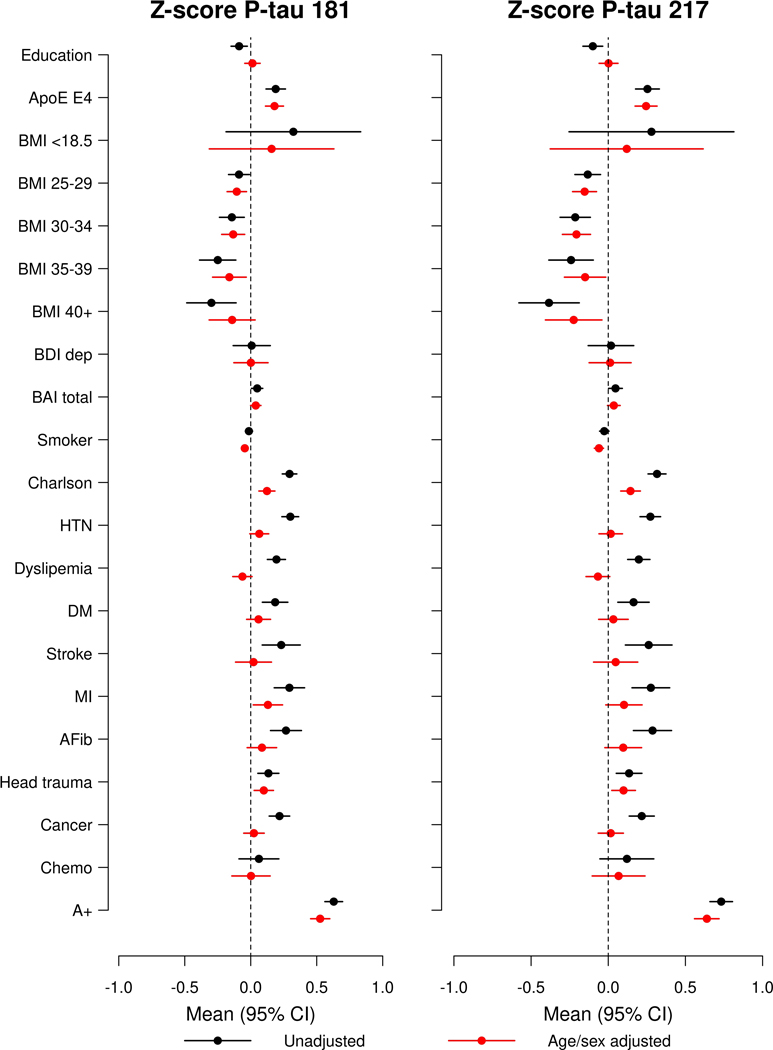
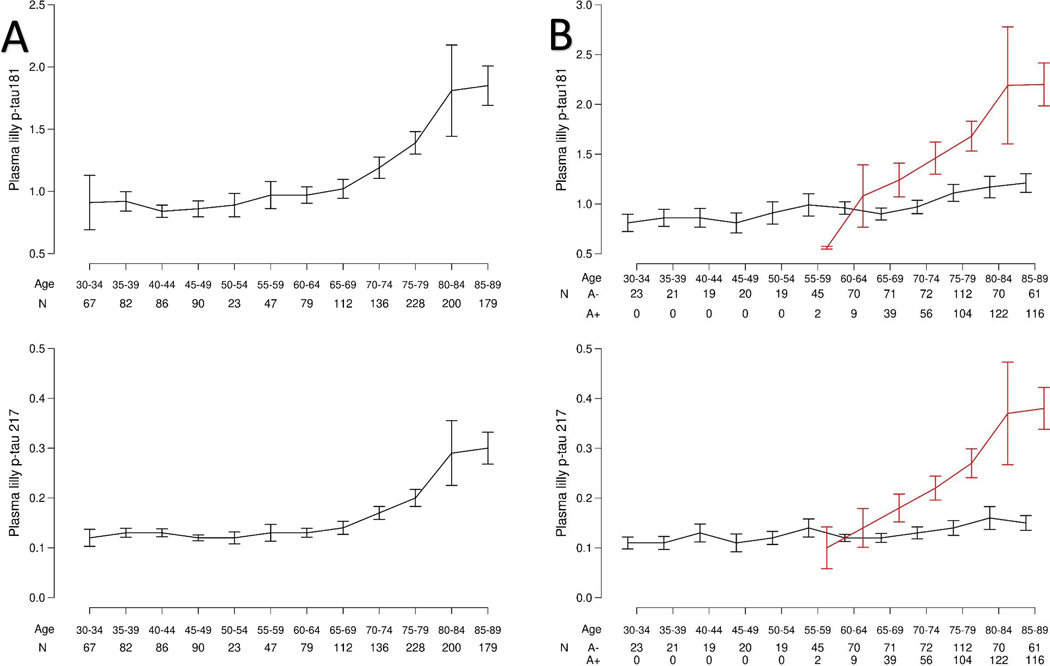
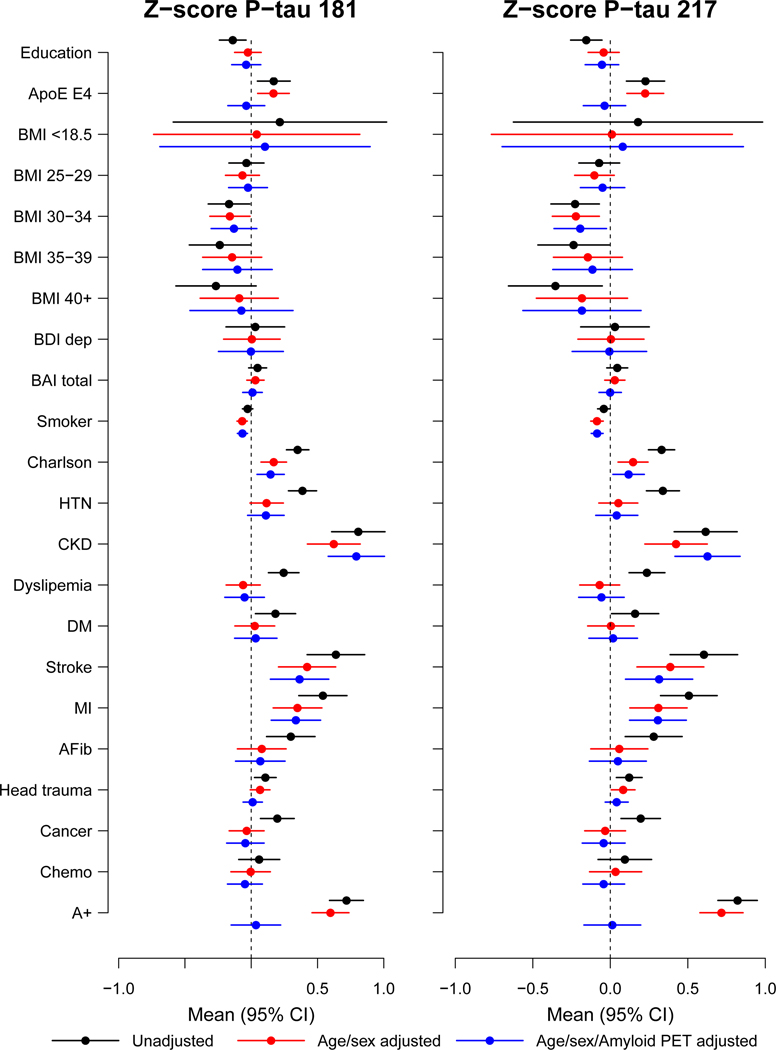
Plasma phosphorylated tau 181 (P-tau181) and 217 (P-tau217) are indicators of both amyloid and tau pathology in clinical settings, but their performance in heterogeneous community-based populations is unclear. We examined P-tau181 and P-tau217 (n = 1,329, aged 30-98 years), in the population-based Mayo Clinic Study of Aging. Continuous, unadjusted plasma P-tau181 and P-tau217 predicted abnormal amyloid positron-emission tomography (PET) (area under the receiver operating characteristic curve (AUROC) = 0.81-0.86) and tau PET entorhinal cortex (AUROC > 0.80), but was less predictive of a tau PET temporal region of interest (AUROC < 0.70). Multiple comorbidities were associated with higher plasma P-tau181 and P-tau217 levels; the difference between participants with and without chronic kidney disease (CKD) was similar to the difference between participants with and without elevated brain amyloid. The exclusion of participants with CKD and other comorbidities affected the establishment of a normal reference range and cutpoints. Understanding the effect of comorbidities on P-tau181 and P-tau217 levels is important for their future interpretation in the context of clinical screening, diagnosis or prognosis at the population level.
© 2022. The Author(s), under exclusive licence to Springer Nature America, Inc.
Figures
Comment in
-
Comorbidities confound Alzheimer's blood tests.Nat Med. 2022 Jul;28(7):1349-1351. doi: 10.1038/s41591-022-01875-3. Nat Med. 2022. PMID: 35788176 No abstract available.
References
-
- Janelidze S. et al. Plasma P-tau181 in Alzheimer’s disease: relationship to other biomarkers, differential diagnosis, neuropathology and longitudinal progression to Alzheimer’s dementia. Nat. Med 26, 379–386 (2020). - PubMed
-
- Karikari TK et al. Blood phosphorylated tau 181 as a biomarker for Alzheimer’s disease: a diagnostic performance and prediction modelling study using data from four prospective cohorts. Lancet Neurol 19, 422–433 (2020). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
