

C-reactive protein elevation predicts in-hospital deterioration after aneurysmal subarachnoid hemorrhage: a retrospective observational study
- PMID: 35618852
- PMCID: PMC9233629
- DOI: 10.1007/s00701-022-05256-0
C-reactive protein elevation predicts in-hospital deterioration after aneurysmal subarachnoid hemorrhage: a retrospective observational study
Abstract
Background: There is increasing evidence that inflammation plays a role in the pathogenesis of aneurysmal subarachnoid hemorrhage (aSAH) and in the development of delayed cerebral ischemia (DCI). However, the assessment and interpretation of classically defined inflammatory parameters is difficult in aSAH patients. The objective of this study was to investigate the relationship between easily assessable findings (hyperventilation, fever, white blood cell count (WBC), and C-reactive protein (CRP)) and the occurrence of DCI and unfavorable neurological outcome at discharge in aSAH patients.
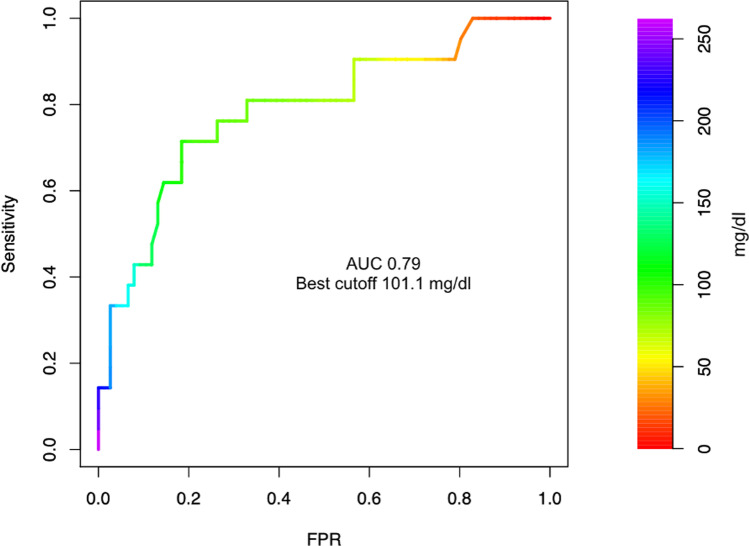
Methods: Retrospective analysis of prospectively collected data from a single center cohort. We evaluated the potential of clinical signs of inflammation (hyperventilation, fever) and simple inflammatory laboratory parameters CRP and WBC to predict unfavorable outcomes at discharge and DCI in a multivariate analysis. A cutoff value for CRP was calculated by Youden's J statistic. Outcome was measured using the modified Rankin score at discharge, with an unfavorable outcome defined as modified Rankin scale (mRS) > 3.
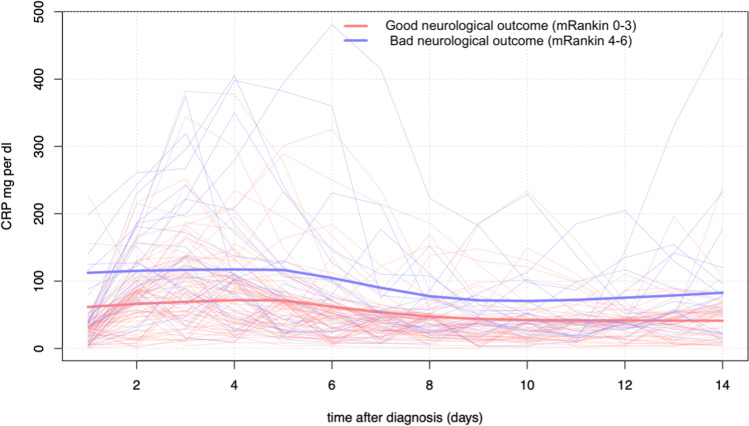
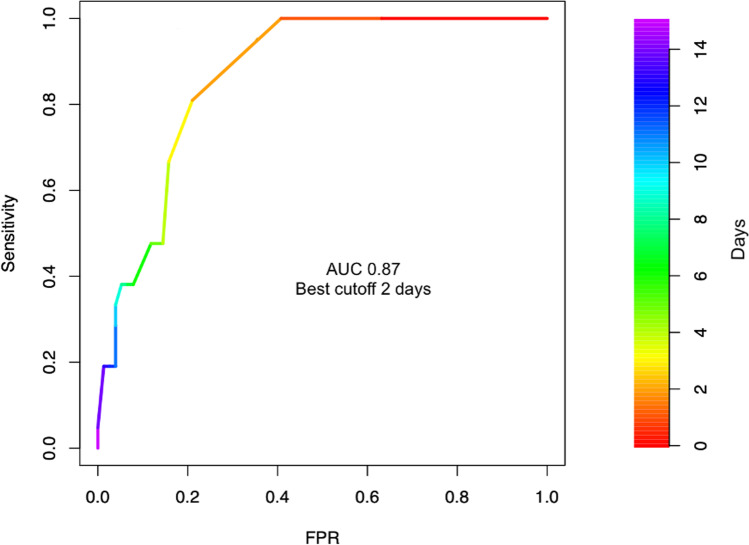
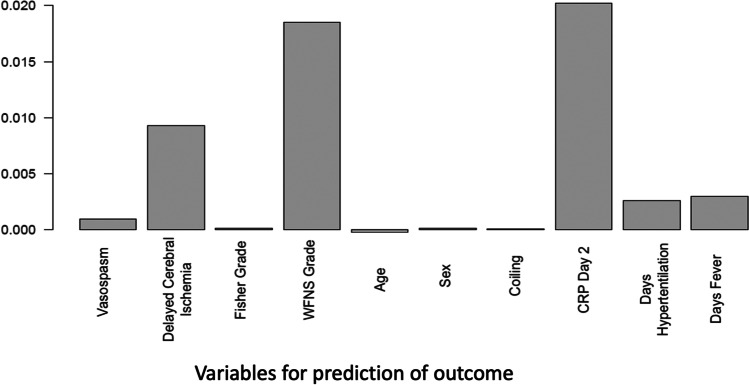
Results: We included 97 consecutive aSAH patients (63 females, 34 males, mean age 58 years) in the analysis. Twenty-one (22%) had major disability or died by the time of hospital discharge. Among inflammatory parameters, CRP over 100 mg/dl on day 2 was an independent predictor for worse neurological outcome at discharge. The average C-reactive protein level in the first 14 days was higher in patients with a worse neurological outcome (96.6, SD 48.3 vs 56.3 mg/dl, SD 28.6) in the first 14 days after aSAH. C-reactive protein on day 2 was an indicator of worse neurological outcome. No inflammatory parameter was an independent predictor of DCI. After multivariate adjustment, DCI, increased age, and more than 1 day of mechanical ventilation were significant predictors of worse neurological outcome.
Conclusions: Early elevated CRP levels were a significant predictor of worse neurological outcome at hospital discharge and may be a useful marker of later deterioration in aSAH.
Keywords: C-reactive protein; Delayed cerebral ischemia; Subarachnoid hemorrhage.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Connolly ES, Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, Hoh BL, Kirkness CJ, Naidech AM, Ogilvy CS, Patel AB, Thompson BG, Vespa P, American Heart Association Stroke C. Council on Cardiovascular R, Intervention. Council on Cardiovascular N. Council on Cardiovascular S, Anesthesia. Council on Clinical C Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43:1711–1737. doi: 10.1161/STR.0b013e3182587839. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
