

Preference Elicitation Techniques Used in Valuing Children's Health-Related Quality-of-Life: A Systematic Review
- PMID: 35619044
- PMCID: PMC9270310
- DOI: 10.1007/s40273-022-01149-3
Preference Elicitation Techniques Used in Valuing Children's Health-Related Quality-of-Life: A Systematic Review
Abstract
Background and objectives: Valuing children's health states for use in economic evaluations is globally relevant and is of particular relevance in jurisdictions where a cost-utility analysis is the preferred form of analysis for decision making. Despite this, the challenges with valuing child health mean that there are many remaining questions for debate about the approach to elicitation of values. The aim of this paper was to identify and describe the methods used to value children's health states and the specific issues that arise in the use of these methods.
Methods: We conducted a systematic search of electronic databases to identify studies published in English since 1990 that used preference elicitation methods to value child and adolescent (under 18 years of age) health states. Eligibility criteria comprised valuation studies concerning both child-specific patient-reported outcome measures and child health states defined in other ways, and methodological studies of valuation approaches that may or may not have yielded a value set algorithm.
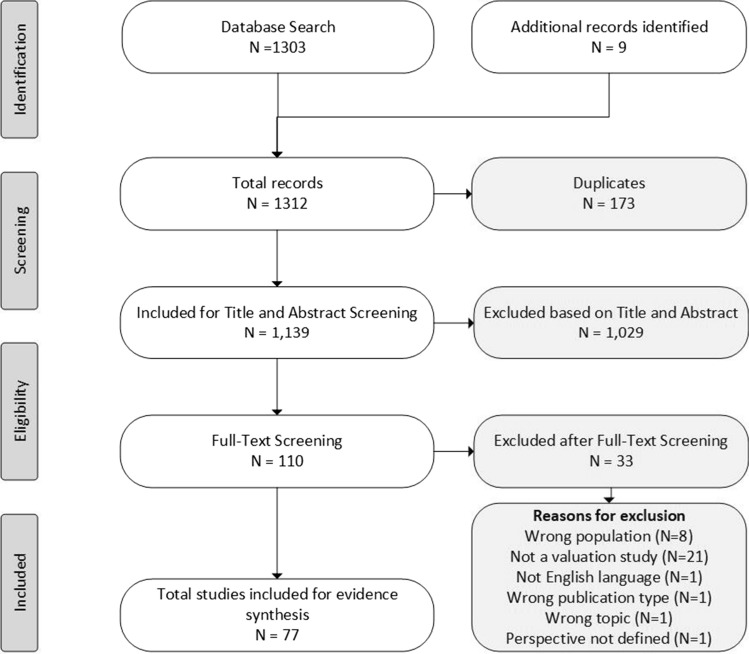
Results: A total of 77 eligible studies were identified from which data on country setting, aims, condition (general population or clinically specific), sample size, age of respondents, the perspective that participants were asked to adopt, source of values (respondents who completed the preference elicitation tasks) and methods questions asked were extracted. Extracted data were classified and evaluated using narrative synthesis methods. The studies were classified into three groups: (1) studies comparing elicitation methods (n = 30); (2) studies comparing perspectives (n = 23); and (3) studies where no comparisons were presented (n = 26); selected studies could fall into more than one group. Overall, the studies varied considerably both in methods used and in reporting. The preference elicitation tasks included time trade-off, standard gamble, visual analogue scaling, rating/ranking, discrete choice experiments, best-worst scaling and willingness to pay elicited through a contingent valuation. Perspectives included adults' considering the health states from their own perspective, adults taking the perspective of a child (own, other, hypothetical) and a child/adolescent taking their own or the perspective of another child. There was some evidence that children gave lower values for comparable health states than did adults that adopted their own perspective or adult/parents that adopted the perspective of children.
Conclusions: Differences in reporting limited the conclusions that can be formed about which methods are most suitable for eliciting preferences for children's health and the influence of differing perspectives and values. Difficulties encountered in drawing conclusions from the data (such as lack of consensus and poor reporting making it difficult for users to choose and interpret available values) suggest that reporting guidelines are required to improve the consistency and quality of reporting of studies that value children's health using preference-based techniques.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest. We note that ND, RV, DJS, RN and BM are members of the EuroQol Group and that ND, RV, DJS, RN, JR, BM, EL and CB have received funding through the EuroQol Group for related research. ND is the Chair of the Board of the EuroQol Research Foundation.
Figures

References
-
- Rowen D, Rivero-Arias O, Devlin N, Ratcliffe J. Review of valuation methods of preference-based measures of health for economic evaluation in child and adolescent populations: where are we now and where are we going? Pharmacoeconomics. 2020;38(4):325–340. doi: 10.1007/s40273-019-00873-7. - DOI - PubMed
-
- Brazier J, Ratcliffe J, Saloman J, Tsuchiya A. Measuring and valuing health benefits for economic evaluation. Oxford: Oxford University Press; 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
